- 130 million infants are born each year, 10% require resuscitation and 3% develop birth asphyxia requiring resuscitation, with 900,000 dying each year. Resuscitation is more often needed for preterm infants.
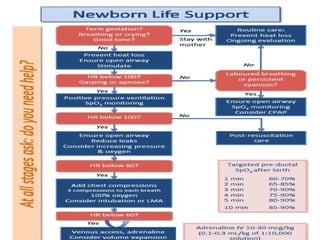
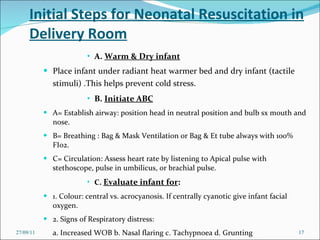
- The goals of resuscitation are to minimize heat loss, establish normal breathing and lung function, increase oxygen levels, and support adequate blood circulation.
- Risk factors for needing resuscitation include maternal infections, illnesses, trauma during delivery, and fetal conditions like meconium in the amniotic fluid or congenital anomalies.
























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)













