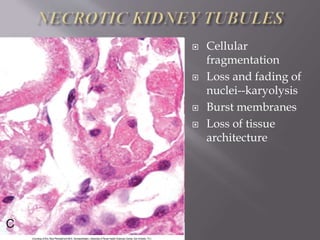
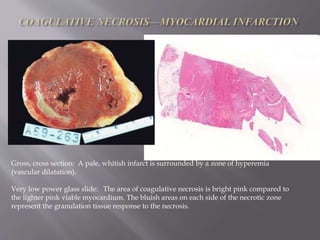
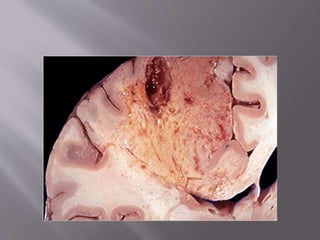
Necrosis refers to cell death and the morphological changes that follow. There are several types of necrosis that can occur depending on the mechanism of cell death, including coagulative, liquefactive, caseous, and gangrenous necrosis. Coagulative necrosis is the most common type and results from ischemia, where the architecture of dead tissue is preserved for weeks before being phagocytosed.