Multiple myeloma is a malignant disease involving clonal expansion of abnormal plasma cells in the bone marrow, leading to various complications such as organ dysfunction, bone disease, and increased susceptibility to infections. It primarily affects older adults with a higher prevalence in males and Black Africans, and the diagnosis requires evidence of paraprotein production, lytic bone lesions, and increased bone marrow plasma cells. Treatment focuses on managing complications, prolonging survival, and supportive care, as the disease remains incurable.
![MULTIPLE MYELOMA
BY DR KD DELE [] DEPT OF INTERNAL MEDICINE](https://image.slidesharecdn.com/multiplemyelomabydrkddele-200318162803/75/Multiple-Myeloma-by-Dr-KD-DELE-1-2048.jpg)
![INTRODUCTION
• Multiple myeloma is a malignant disease of the plasma cells of
bone marrow that is characterized by
• Clonal expansion of abnormal, proliferating plasma cells in the
bone marrow microenvironment – replacing the marrow,
• Production of monoclonal paraproteinemia [i.e. abnormal Ig,
mainly IgG (60%) or IgA (20%) and rarely IgM and IgD, IgE]
• and/or excretion of the monoclonal paraprotein in the urine
(20% cases)
• and associated organ dysfunction
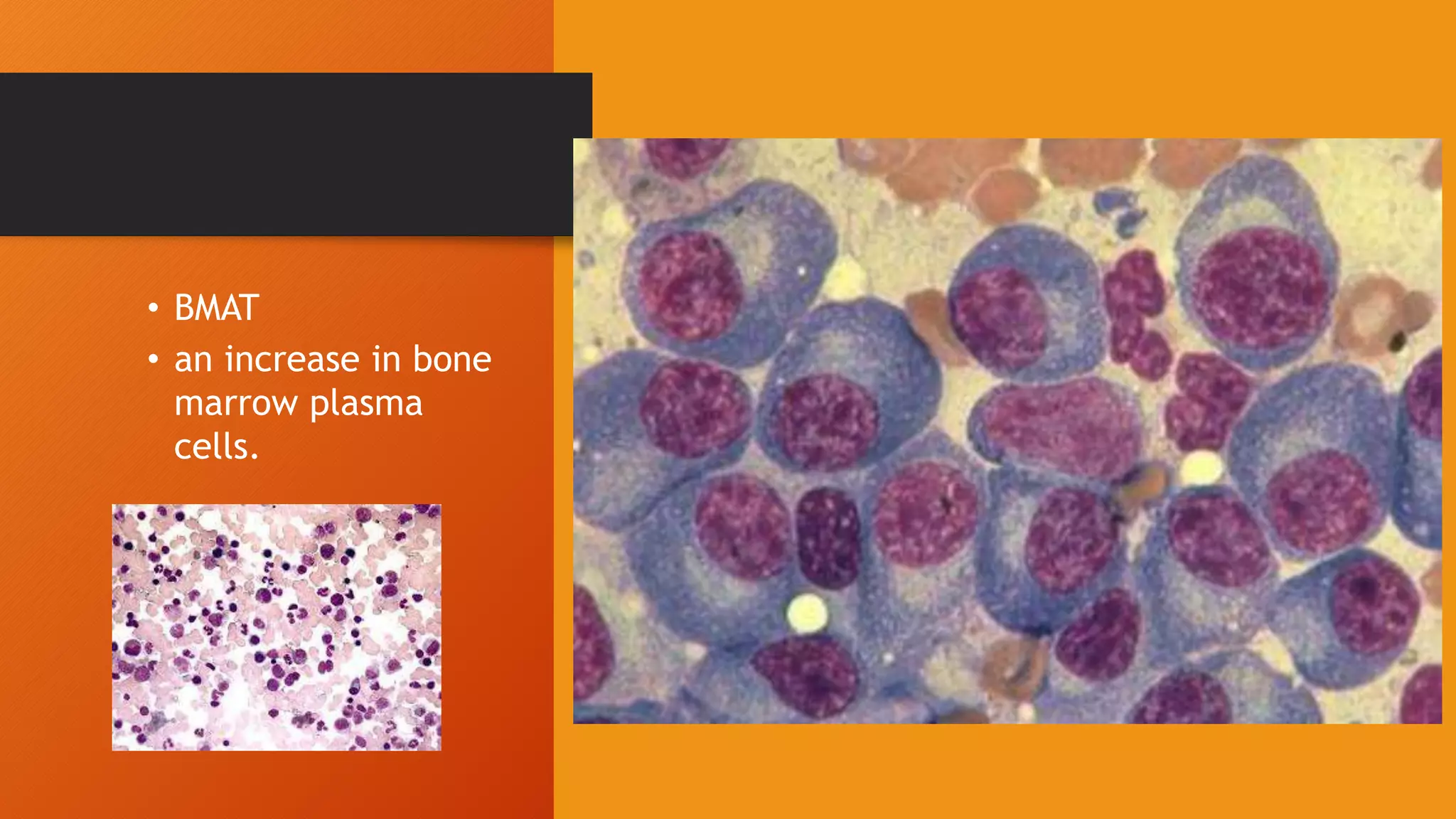
Plasma cells: a fully differentiated b lymphocyte cell](https://image.slidesharecdn.com/multiplemyelomabydrkddele-200318162803/75/Multiple-Myeloma-by-Dr-KD-DELE-2-2048.jpg)














![INVESTIGATIONS: IMMUNOLOGY
• Serum protein electrophoresis (PEP): detects paraprotein in
serum. It characteristically shows a monoclonal band.
• Immunofixation electrophoresis (IEE): detects paraprotein in
serum. reveals it to be a monoclonal immunoglobulin.
• Serum free light chain assay: 15% of patients will have no
demonstrable paraprotein in the serum because their myeloma
cells produce only light chains and not intact immunoglobulin
• Urine PEP/IEE: [excretion of light chains paraprotein i.e. Bence
Jones protein – either kappa or lambda].](https://image.slidesharecdn.com/multiplemyelomabydrkddele-200318162803/75/Multiple-Myeloma-by-Dr-KD-DELE-19-2048.jpg)
![INVESTIGATIONS: IMMUNOLOGY
• 24-hour urine electrophoresis and immunofixation is used for
assessment of light-chain excretion.
• Urine PEP/IEE:
• excretion of light chains paraprotein i.e. Bence Jones protein –
either kappa or lambda].](https://image.slidesharecdn.com/multiplemyelomabydrkddele-200318162803/75/Multiple-Myeloma-by-Dr-KD-DELE-20-2048.jpg)