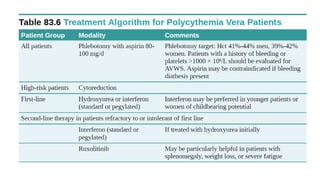
Polycythemia vera is a chronic myeloproliferative disorder characterized by an absolute increase in red blood cells, total blood volume, leukocytosis, thrombocytosis, and splenomegaly. It is caused by a clonal proliferation of a hematopoietic stem cell. Symptoms include headaches, visual disturbances, thrombosis, pruritus, and splenomegaly. Diagnosis involves meeting certain criteria including elevated hematocrit. Treatment involves phlebotomy to reduce red blood cell mass and hydroxyurea or interferon-alpha to reduce platelet and white blood cell counts and reduce risk of thrombosis.