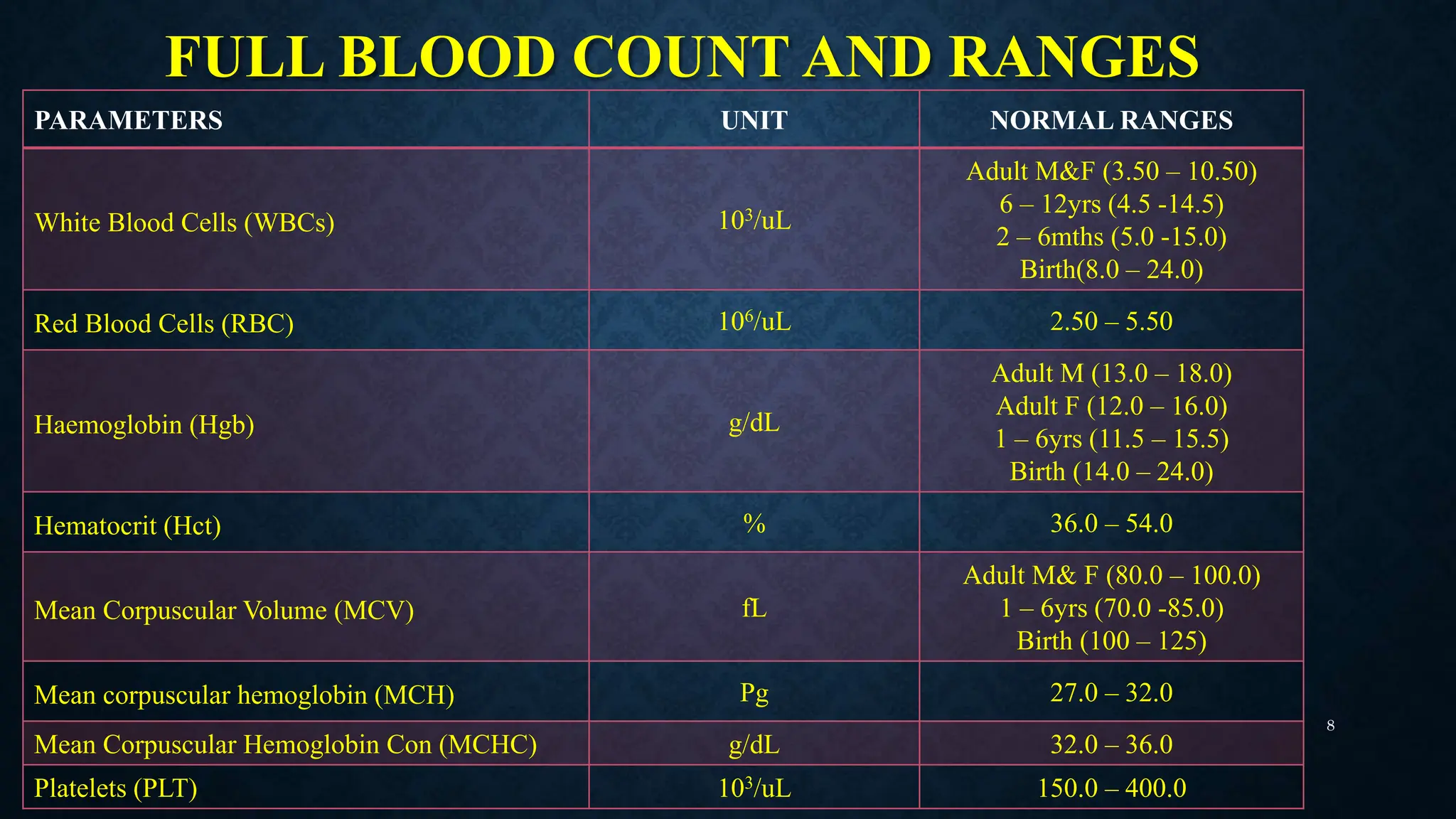
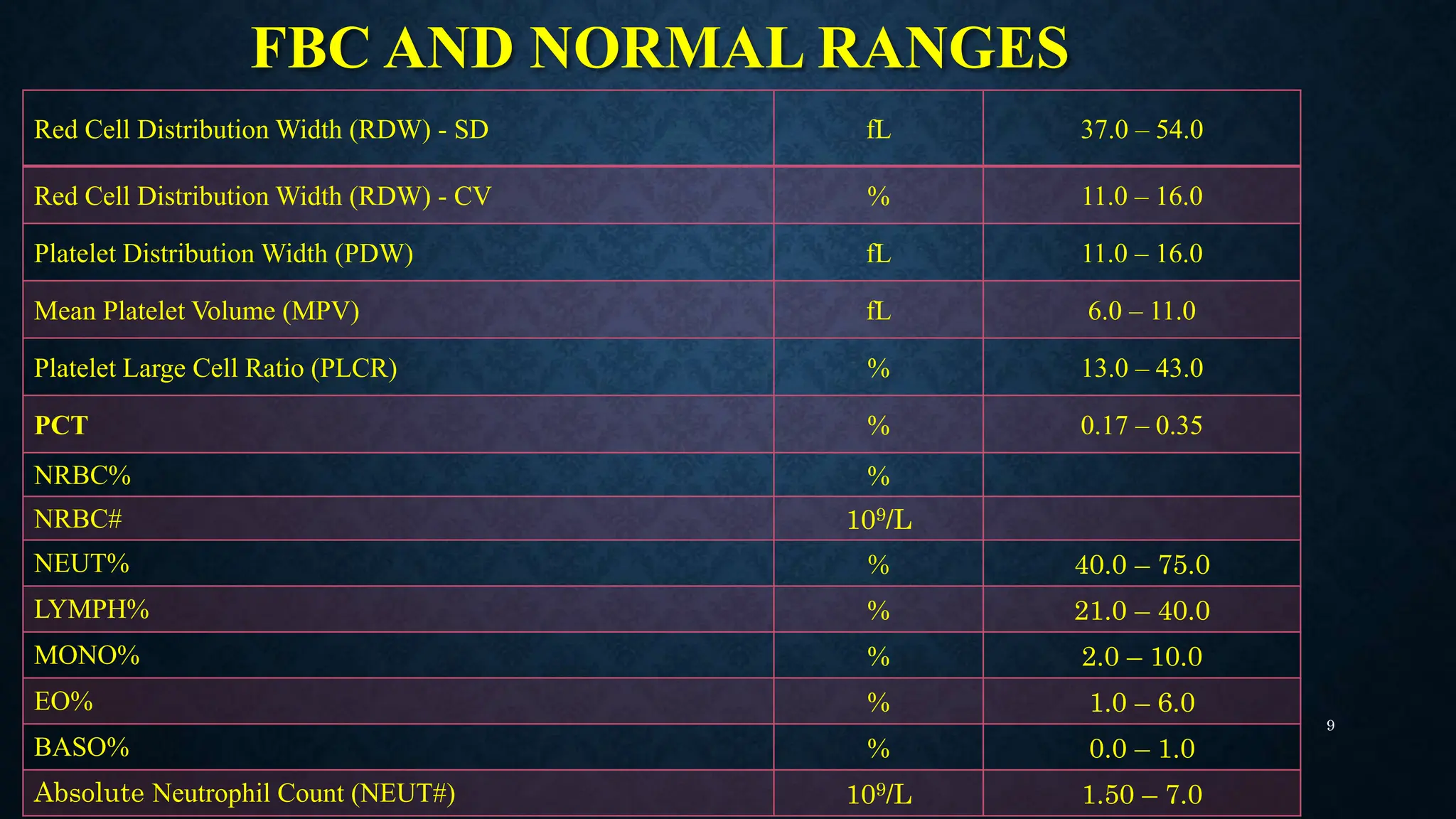
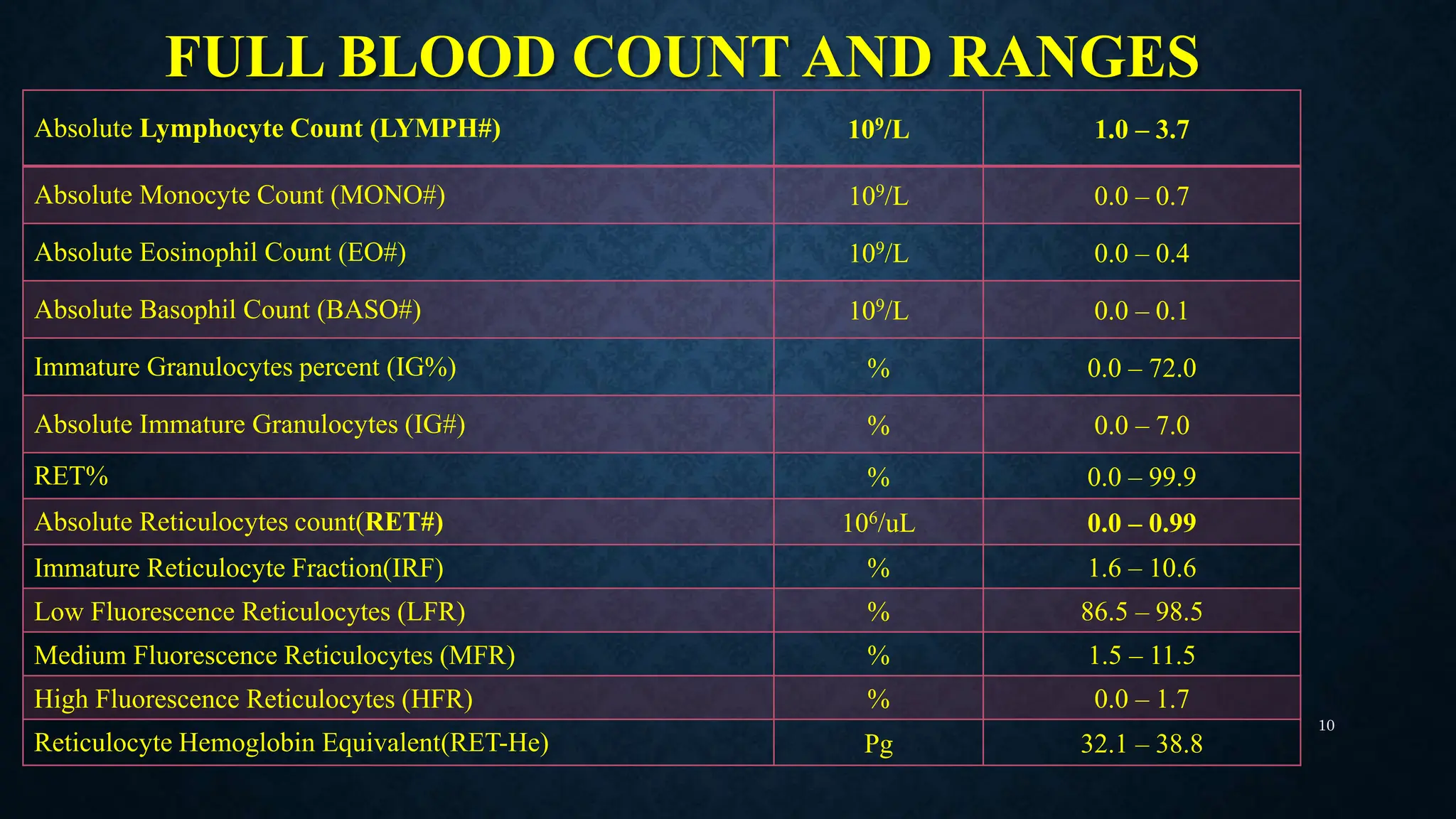
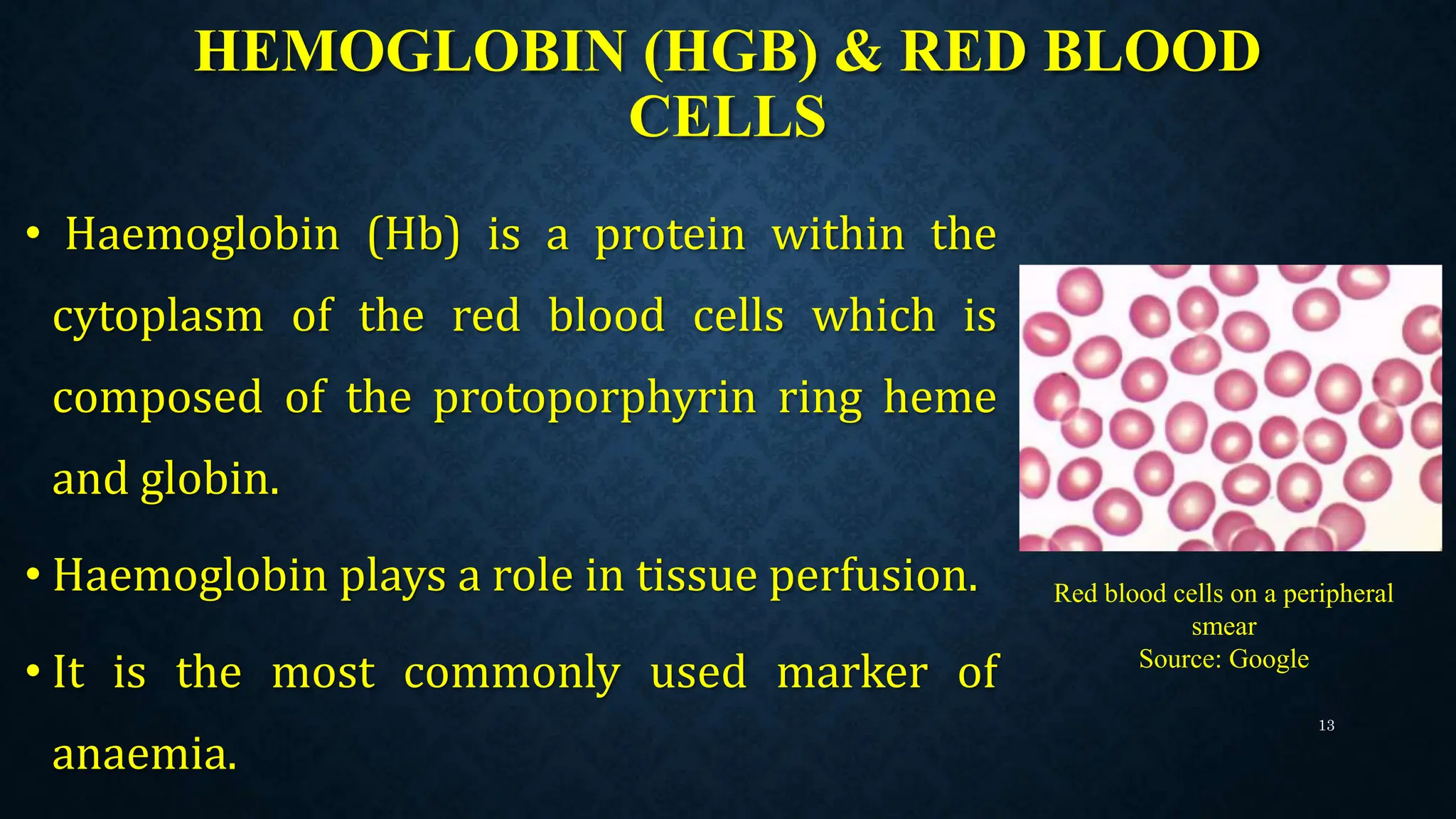
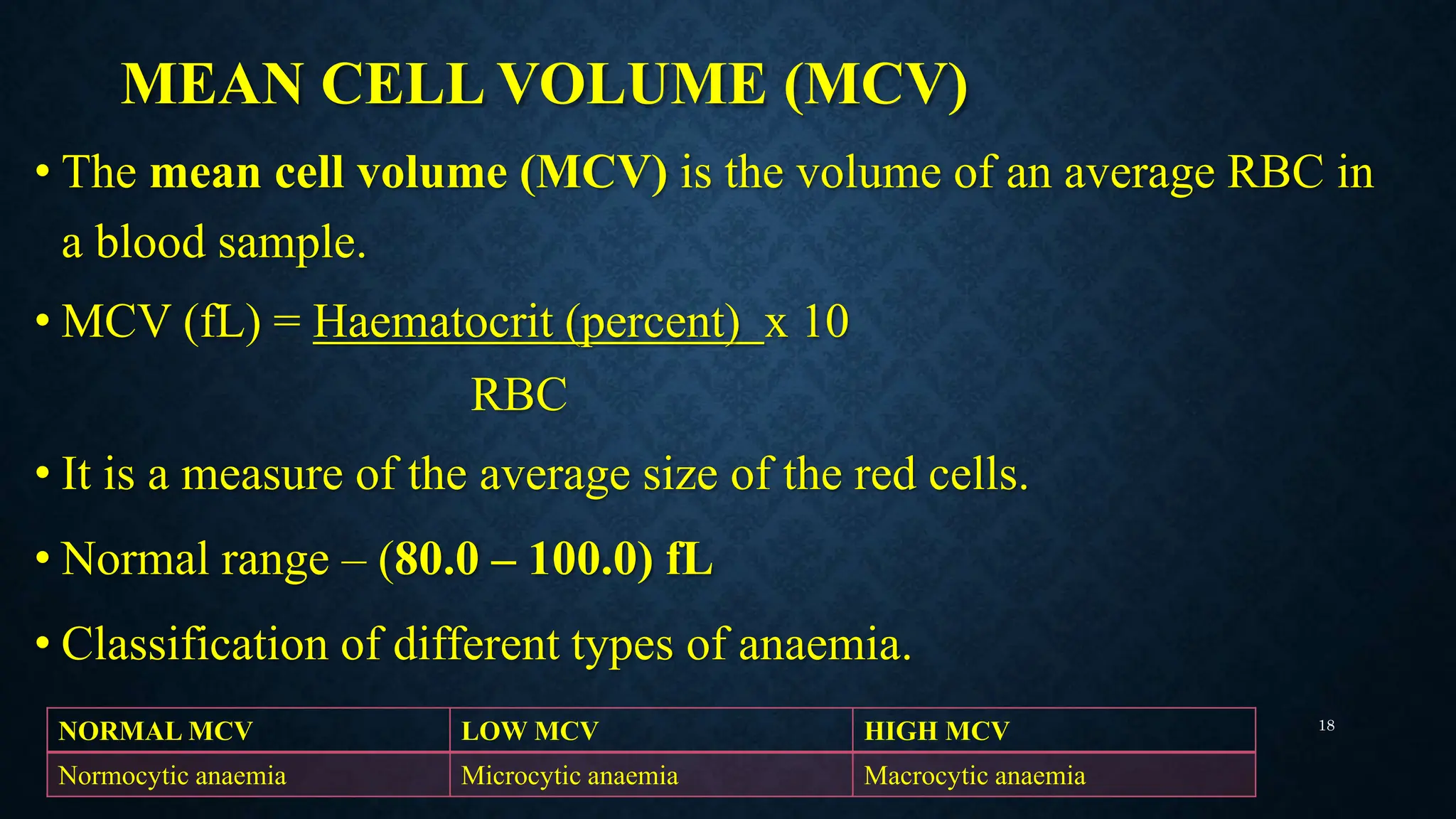
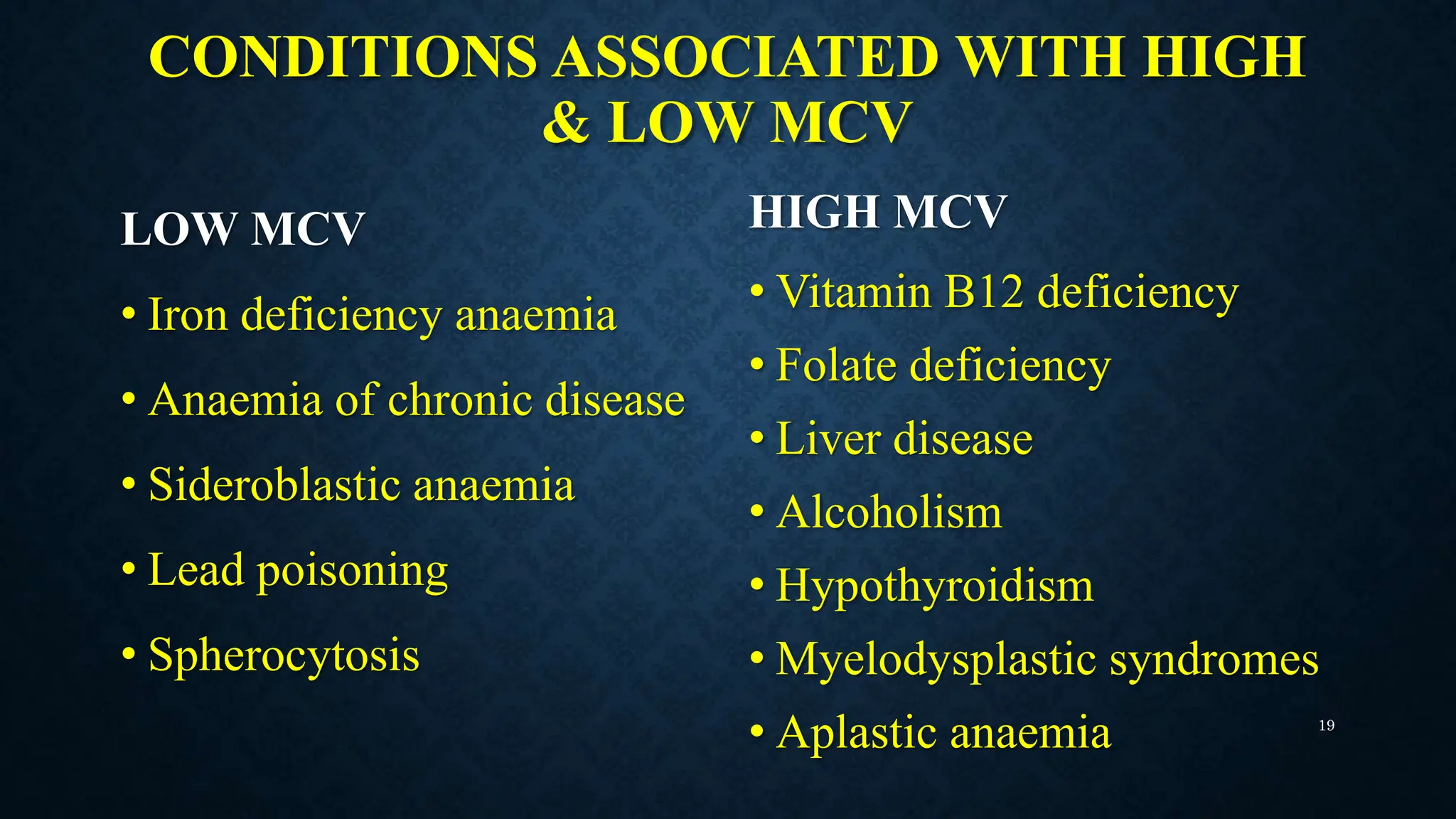
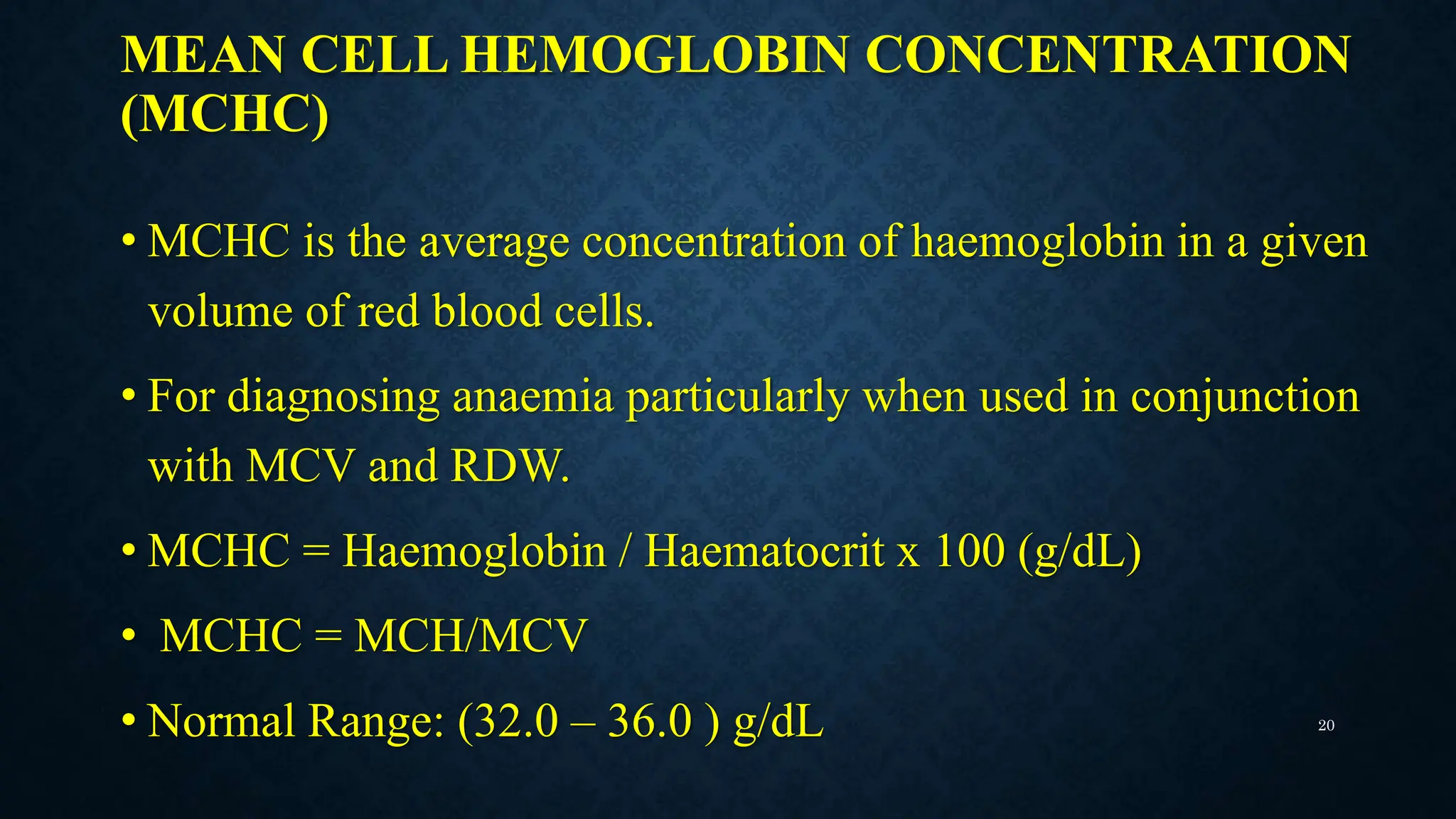
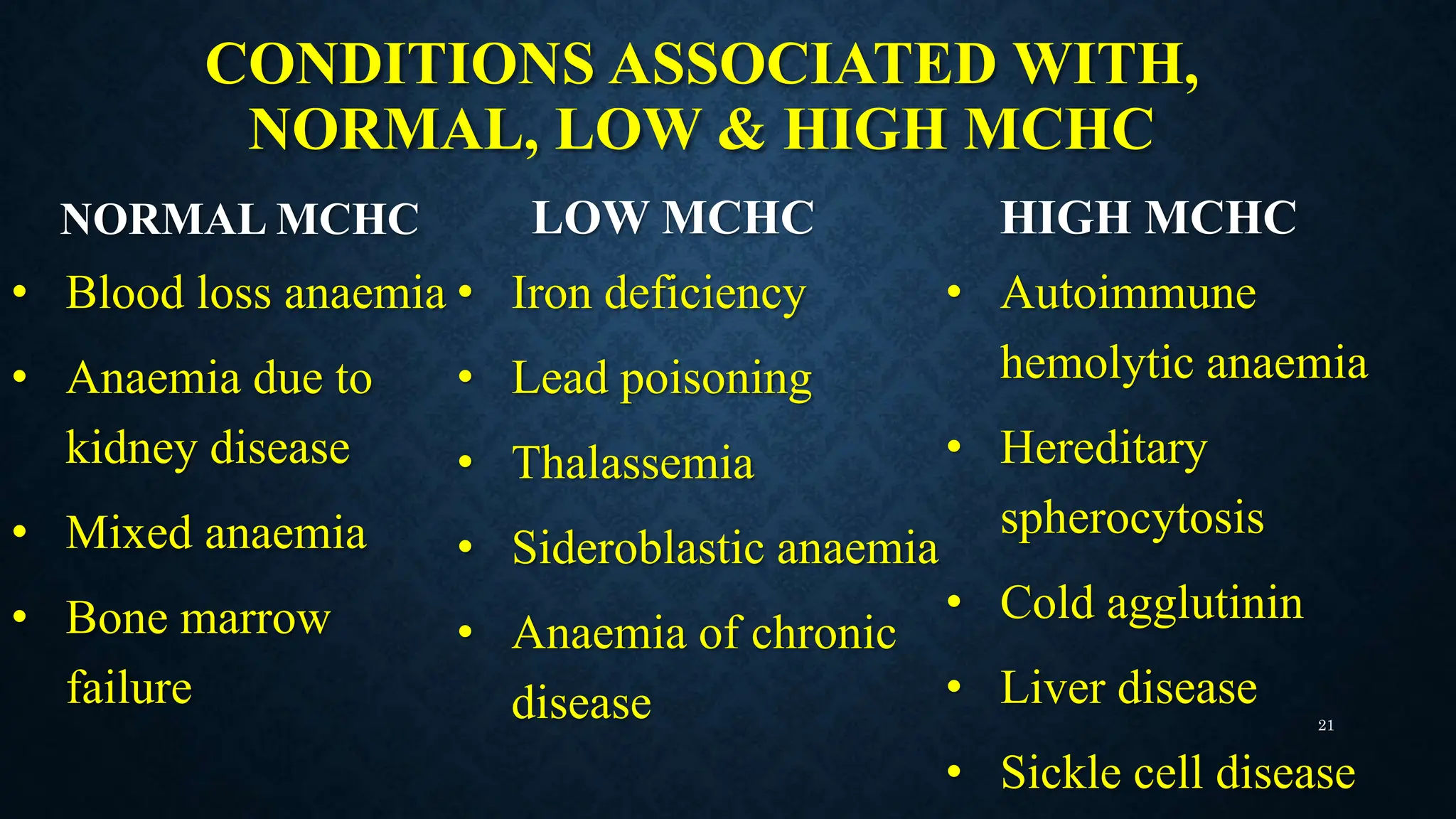
The document provides an in-depth presentation on the interpretation of full blood count (FBC) tests, detailing the components measured including red blood cells, white blood cells, and platelets, along with their significance in diagnosing various medical conditions. It outlines methods for obtaining FBC results, normal ranges for blood parameters, and interpretations related to specific disorders such as anemia and infections. The conclusion emphasizes the necessity for healthcare personnel to accurately interpret FBC results in clinical practice.