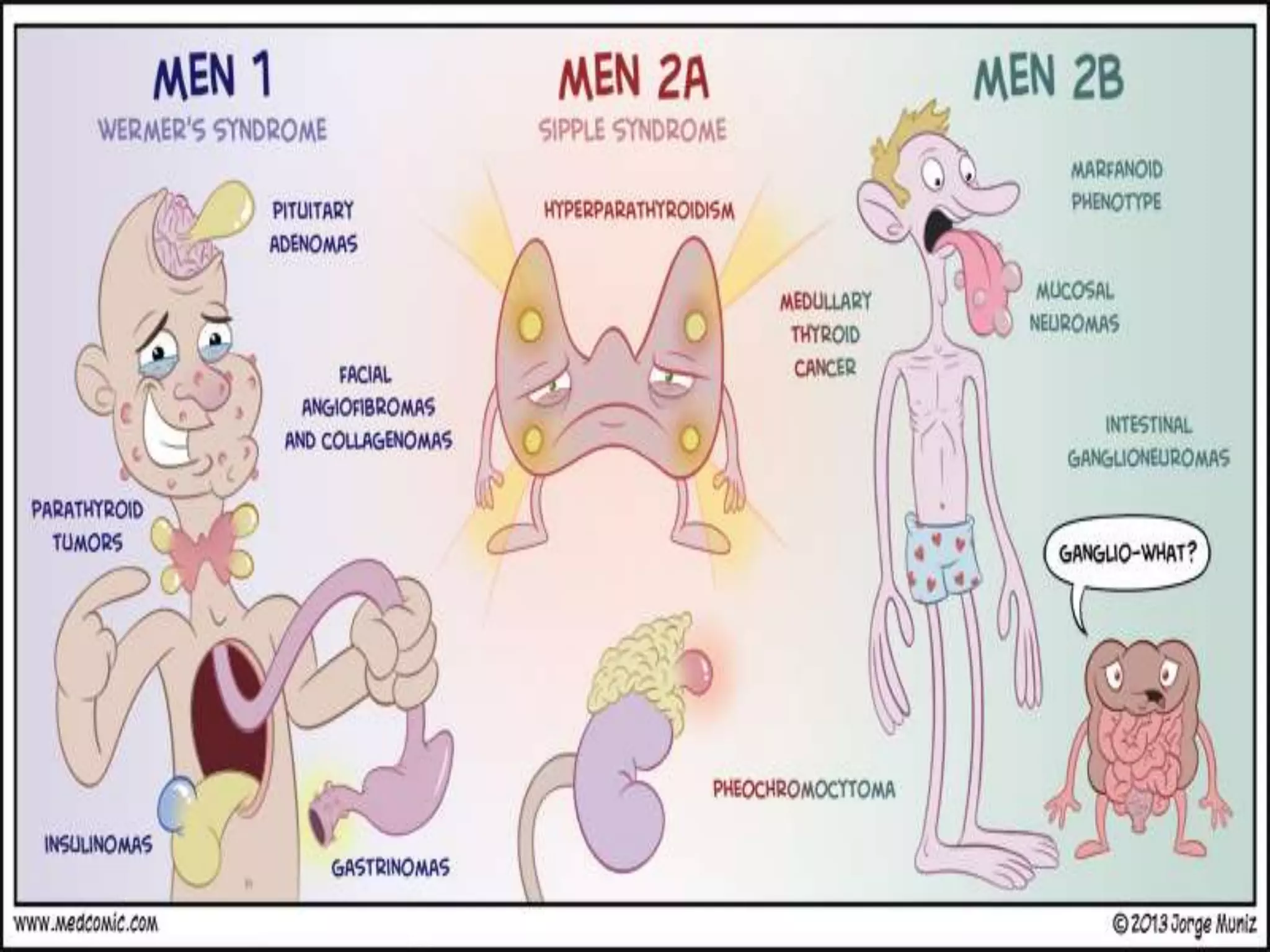
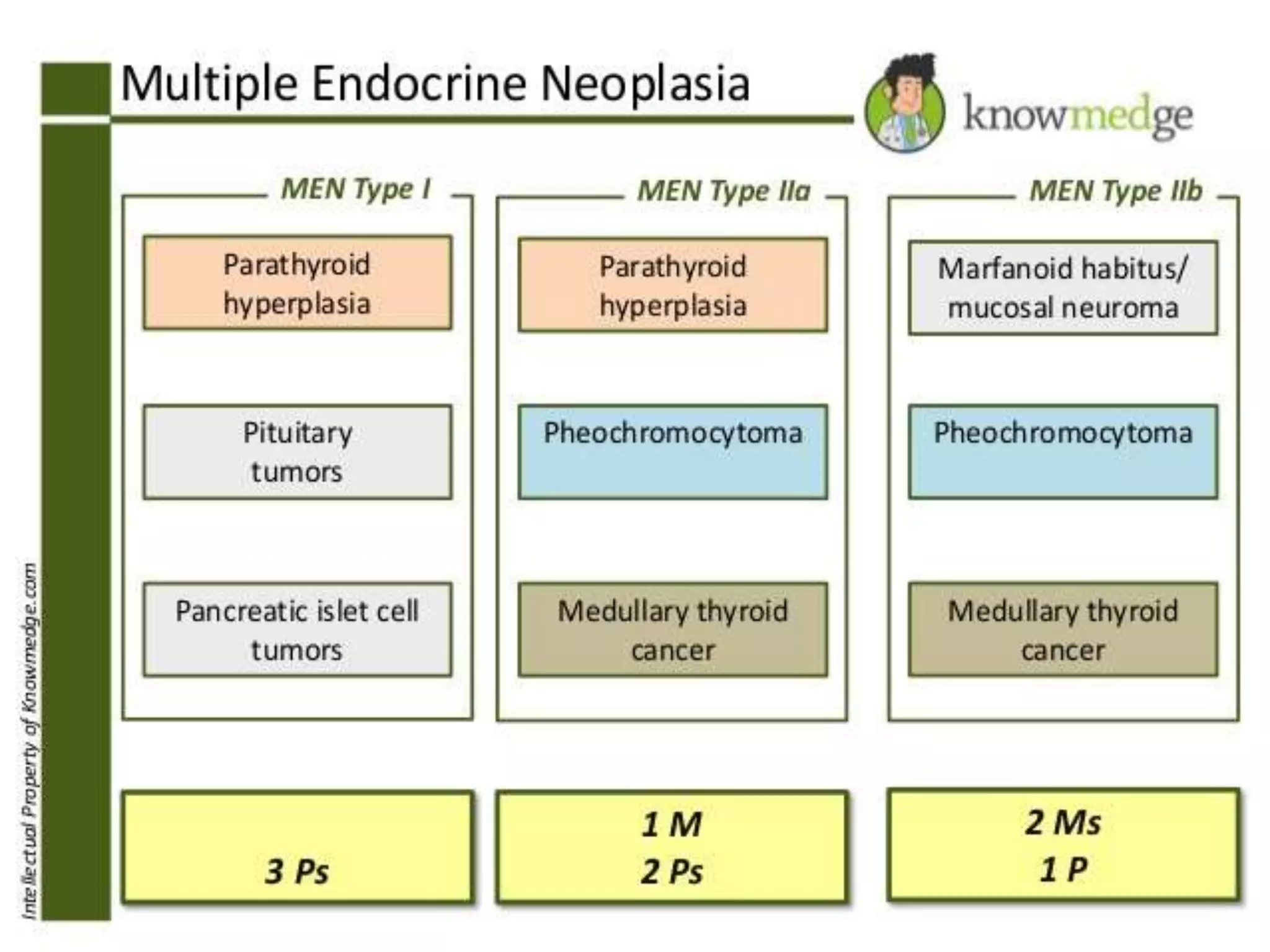
Multiple endocrine neoplasia (MEN) type 1 is characterized by tumors of the parathyroid glands, pancreas, and pituitary gland. It is caused by mutations in the MEN1 gene which codes for the menin protein. Patients with MEN1 often present with hyperparathyroidism, pancreatic neuroendocrine tumors, or prolactin-secreting pituitary adenomas. Diagnosis involves blood tests and imaging to identify affected organs. Treatment depends on the specific tumors but may include parathyroidectomy, surgical removal of pancreatic tumors, and medication for functional tumors. Ongoing screening is important due to the risk of additional tumors developing over time.




![Pancreatic polypeptidomas (PPomas)
Pancreatic polypeptide levels are elevated.
Chromogranin A levels can be elevated in any pancreatic
neuroendocrine tumor.
Screening should begin by age 10 years.
Carcinoid tumors
Elevated levels of chromogranin A, calcitonin, corticotropin, or
urinary 5-hydroxyindoleacetic acid (5-HIAA) can occur.
screening is dependent on radiological imaging as no
biochemical abnormality has been consistently observed.
Pituitary tumors
Assess growth hormone levels (insulinlike growth factor-1 [IGF-
1]) and prolactin.
Screening should begin by age 5 years.
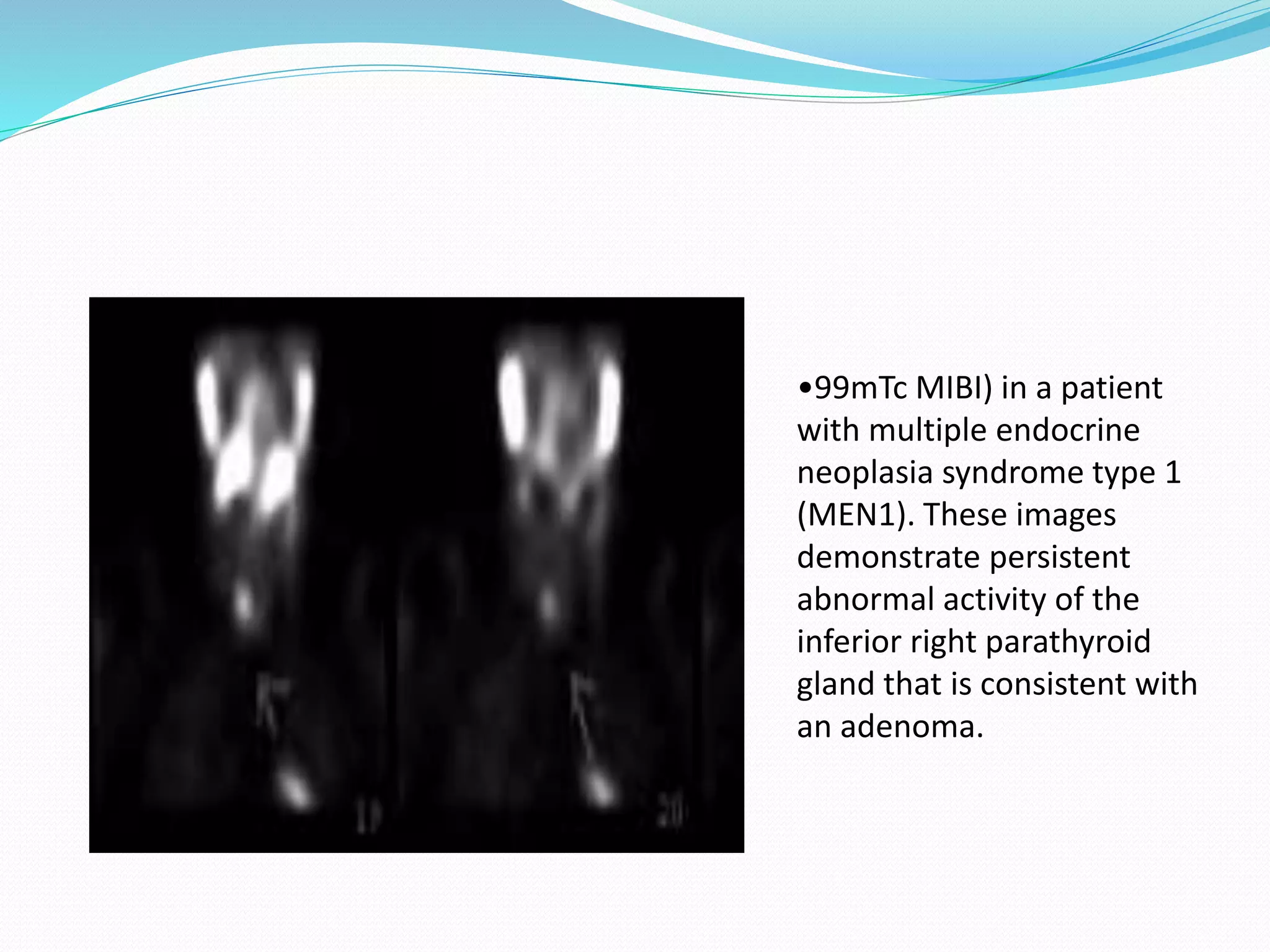
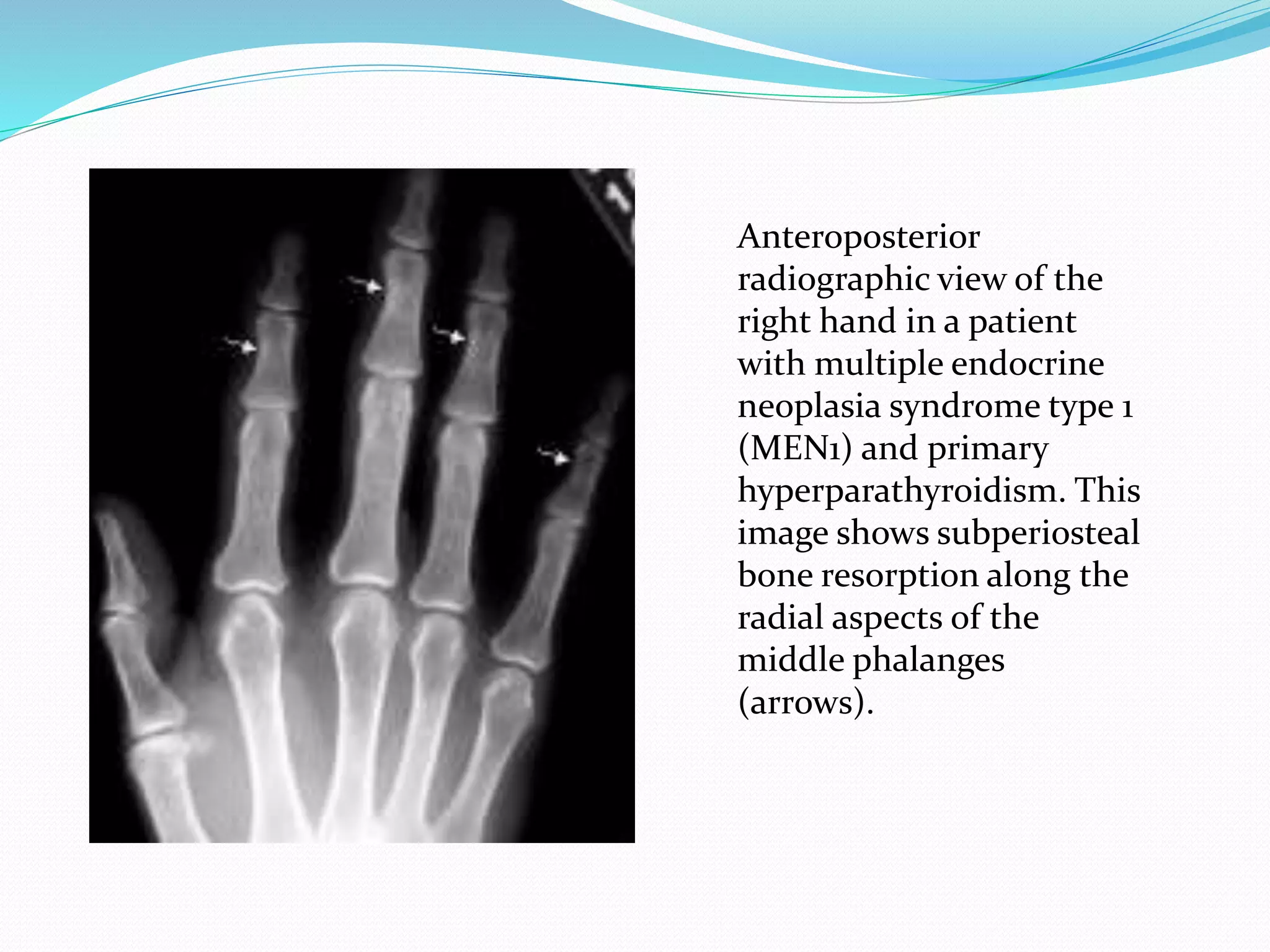
Hyperparathyroidism
Calcium is elevated with an inappropriately elevated parathyroid
hormone level.
Screening should start by age 8 years.](https://image.slidesharecdn.com/multipleendocrineneoplasiamensyndromes-180316184612/75/Multiple-endocrine-neoplasia-men-syndromes-19-2048.jpg)