Downloaded 53 times







































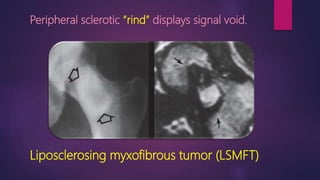
![Rind sign
Fibrous dysplasia
[Layer of thick, sclerotic reactive bone (rind)]](https://image.slidesharecdn.com/msksigns-edited-191223132115/85/Msk-signs-edited-43-320.jpg)

































































































































This document contains medical images and descriptions of various musculoskeletal signs and pathologies. It discusses imaging findings and classifications for conditions like: - Adhesive capsulitis showing thickened ligaments. - SLAC and SNAC wrist classifications. - Femoroacetabular impingement presentations. - Charcot neuroarthropathy acute and chronic stages. - Various tendon injuries and ligamentous injuries patterns. It provides comparisons of imaging findings between similar conditions like fibrous dysplasia and osteofibrous dysplasia. Assessment techniques for foot deformities like clubfoot and flatfoot are also outlined.