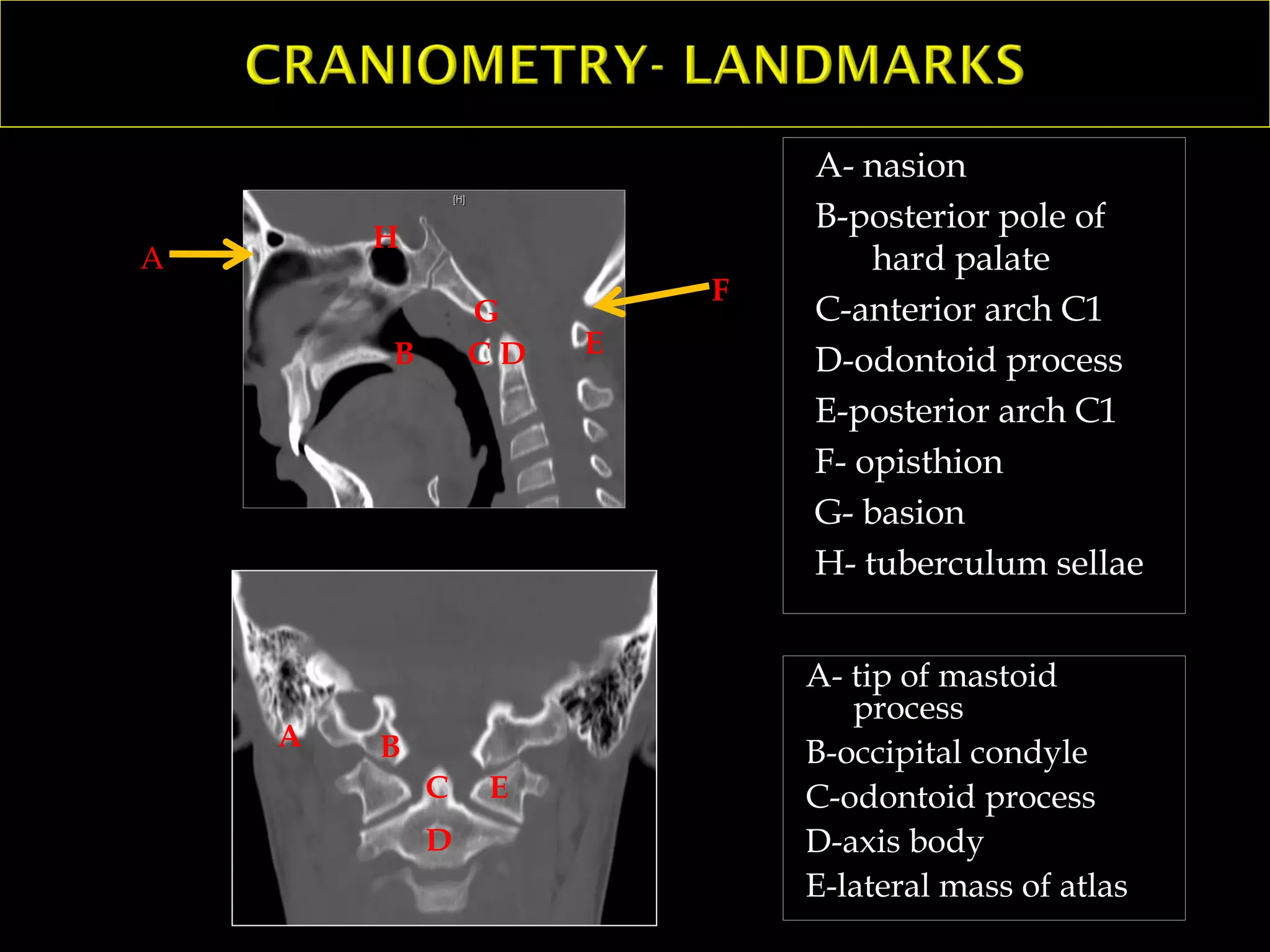
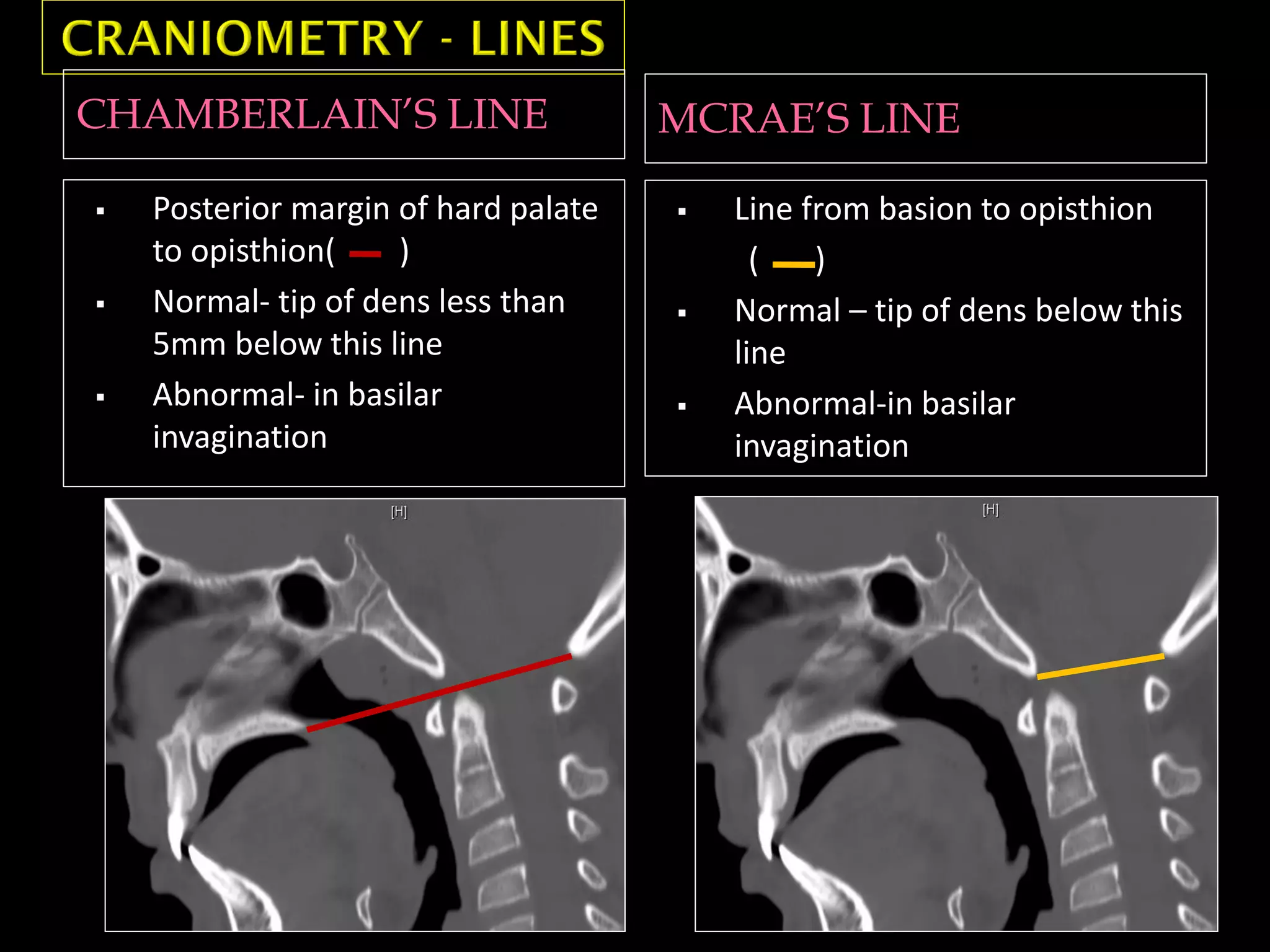
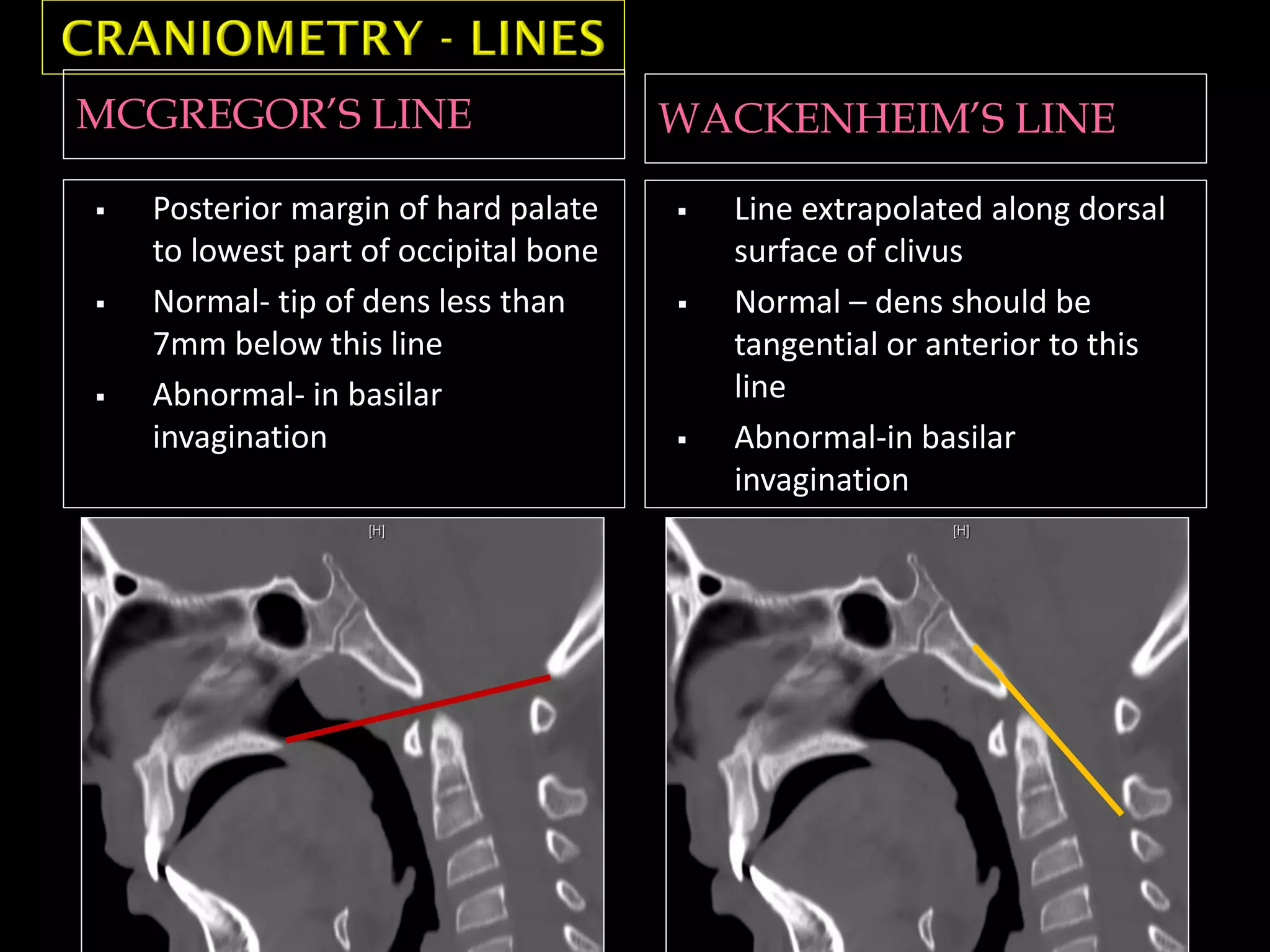
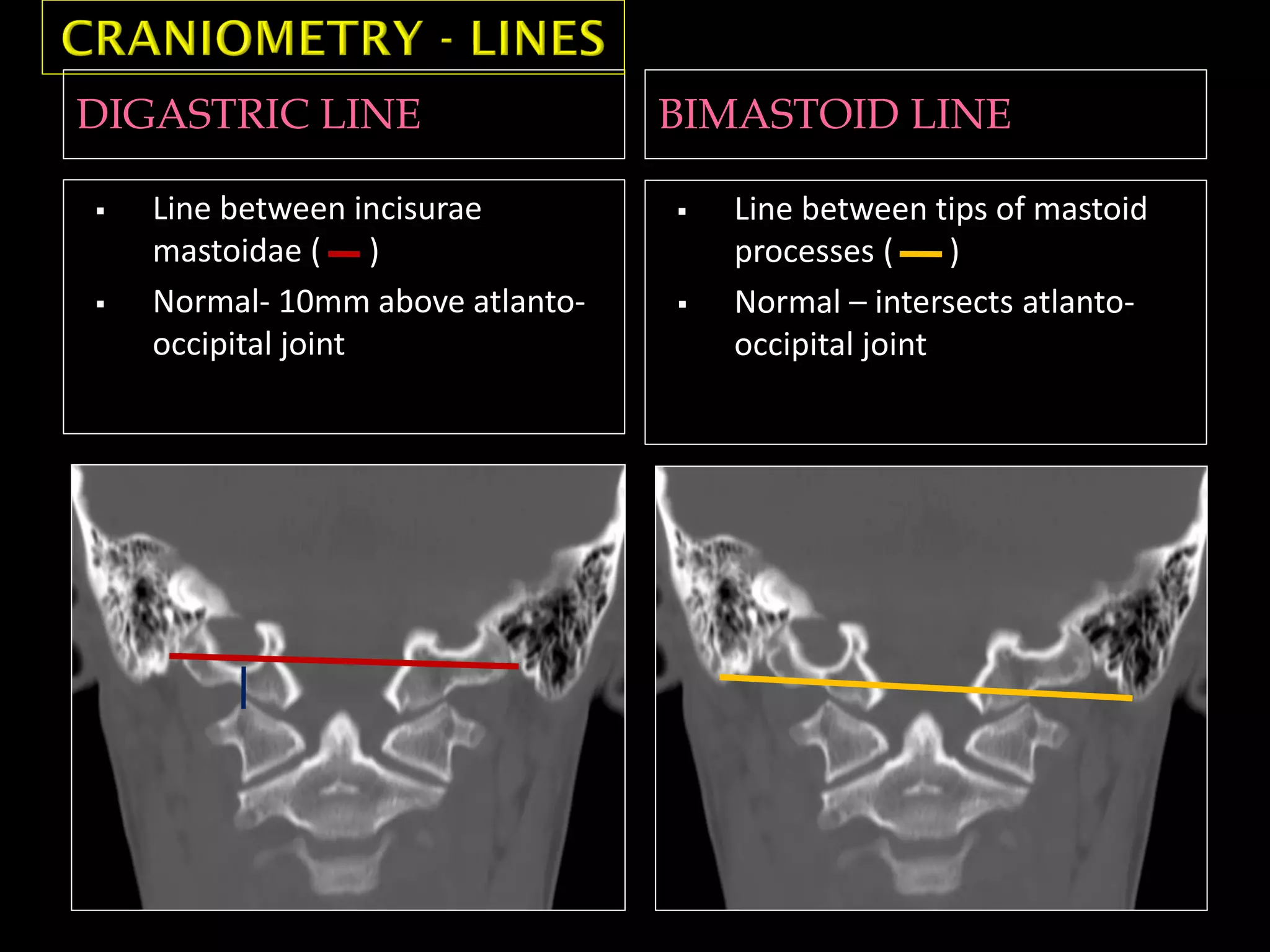
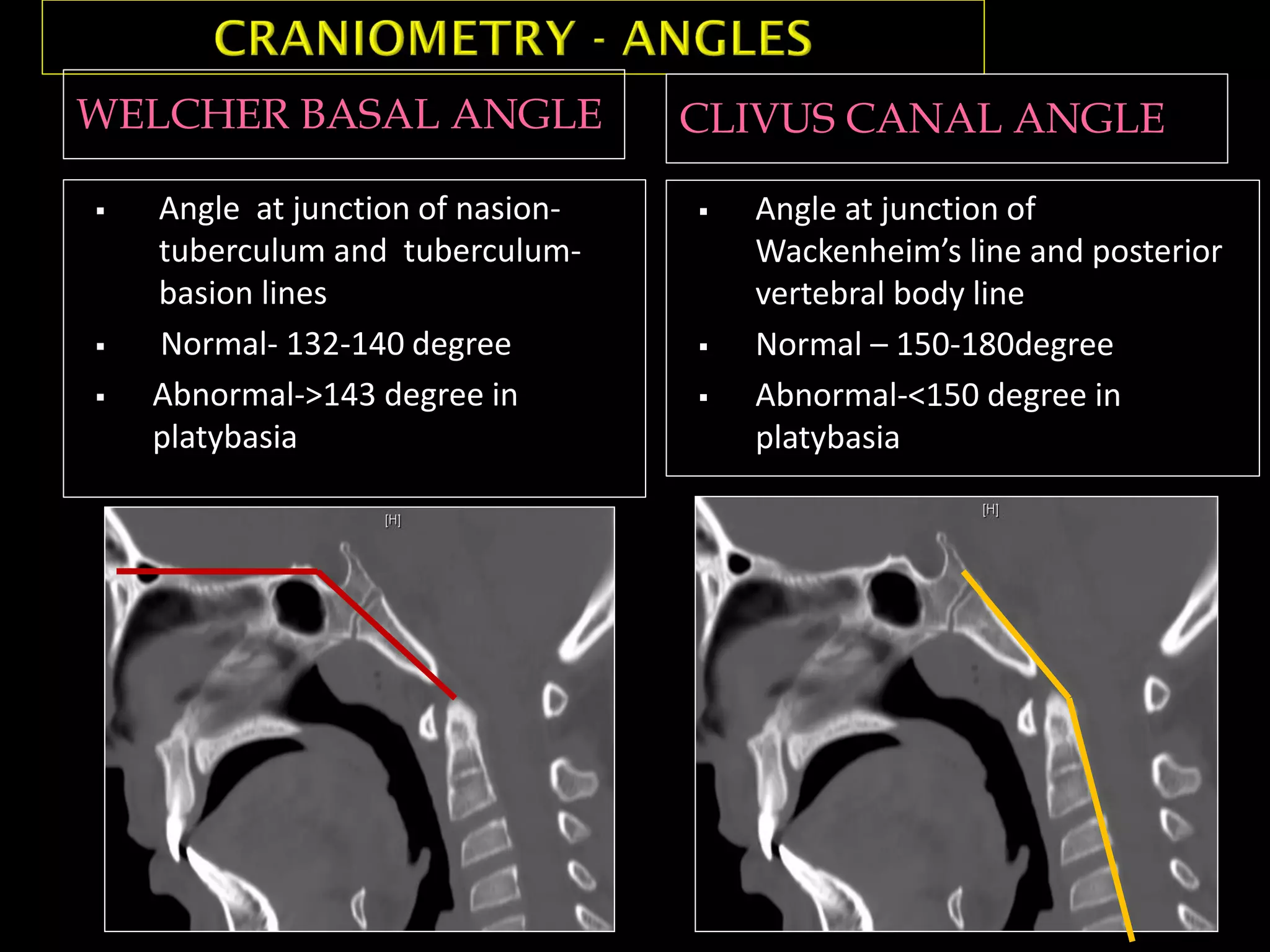
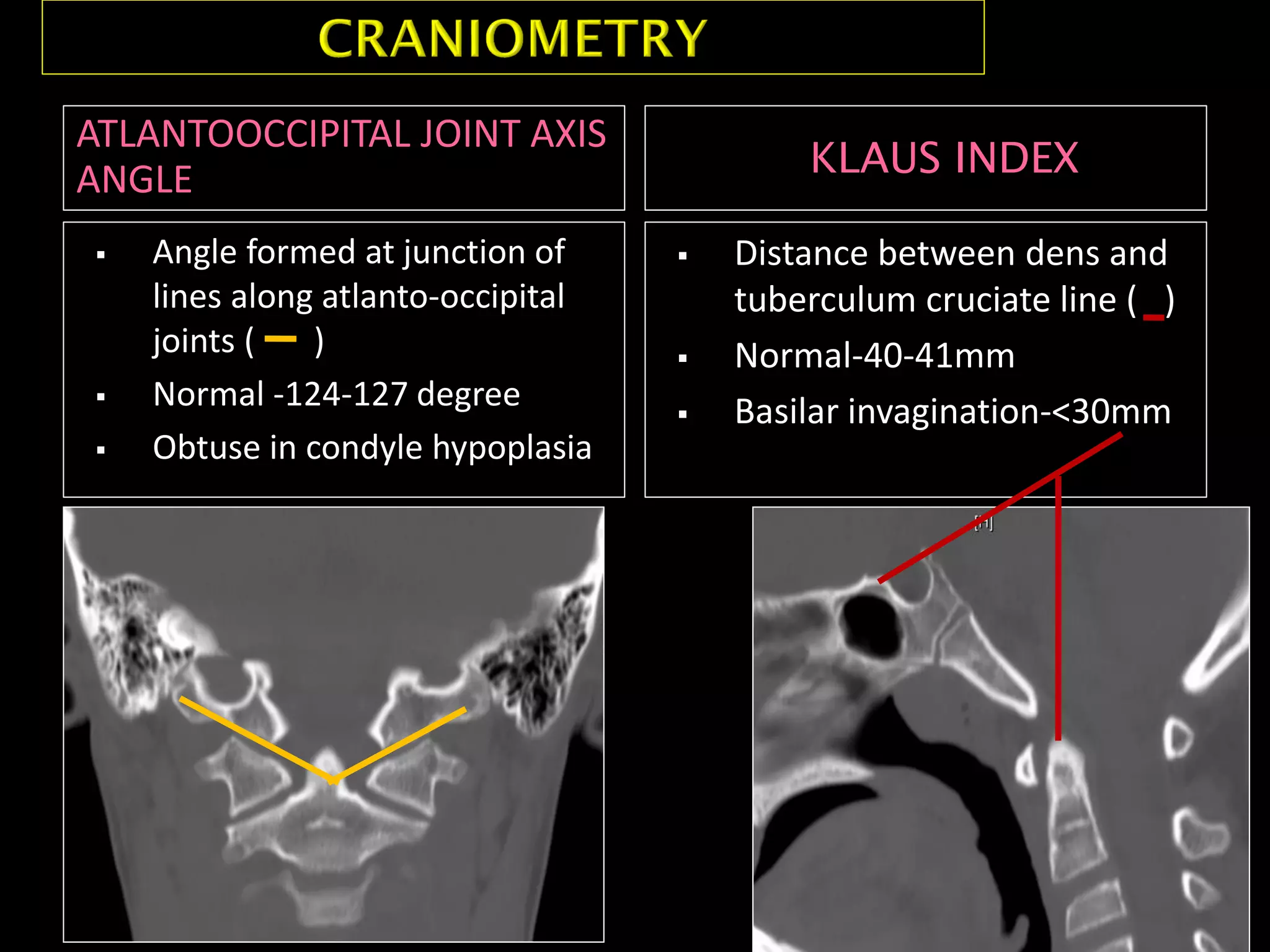
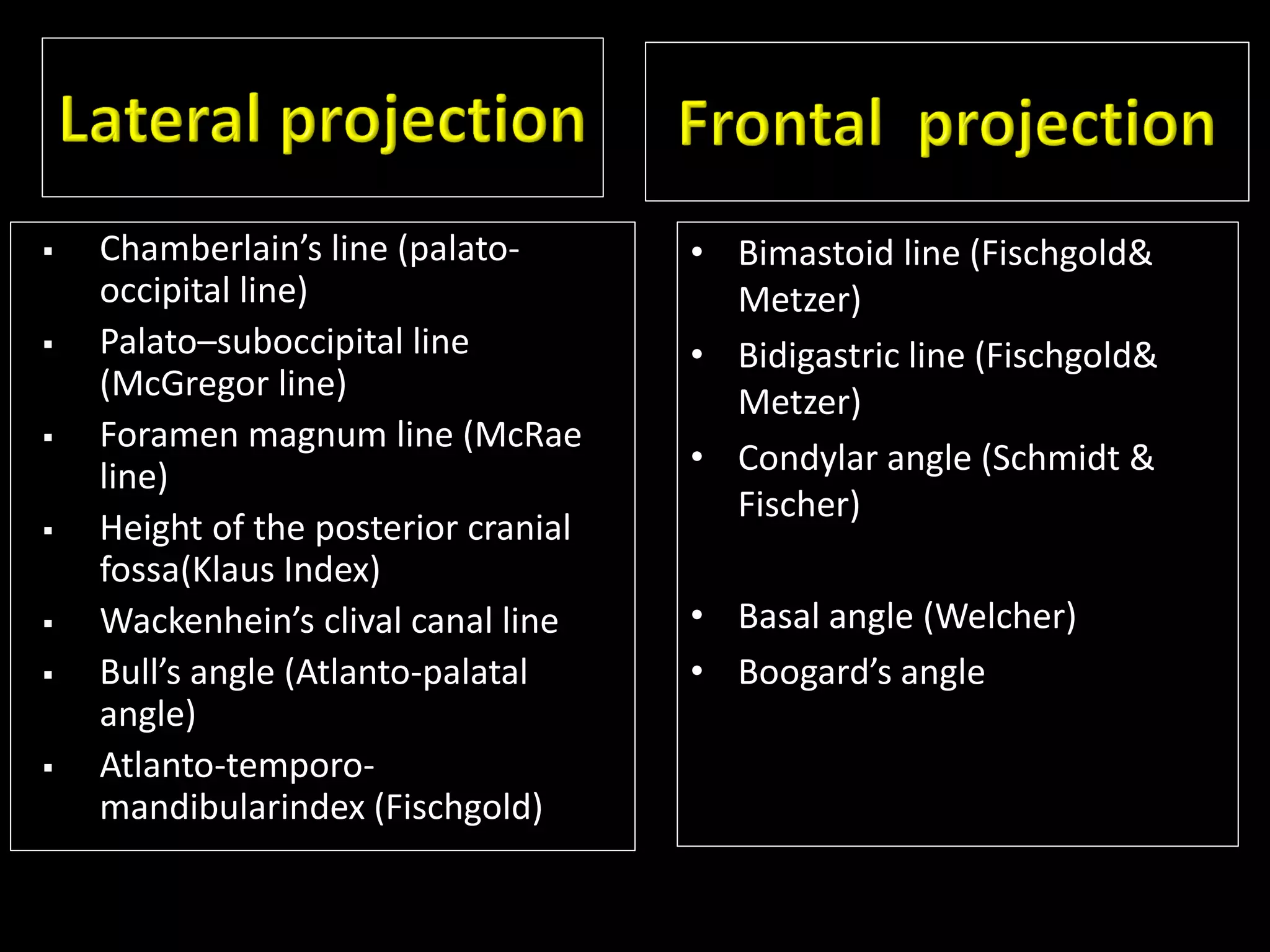
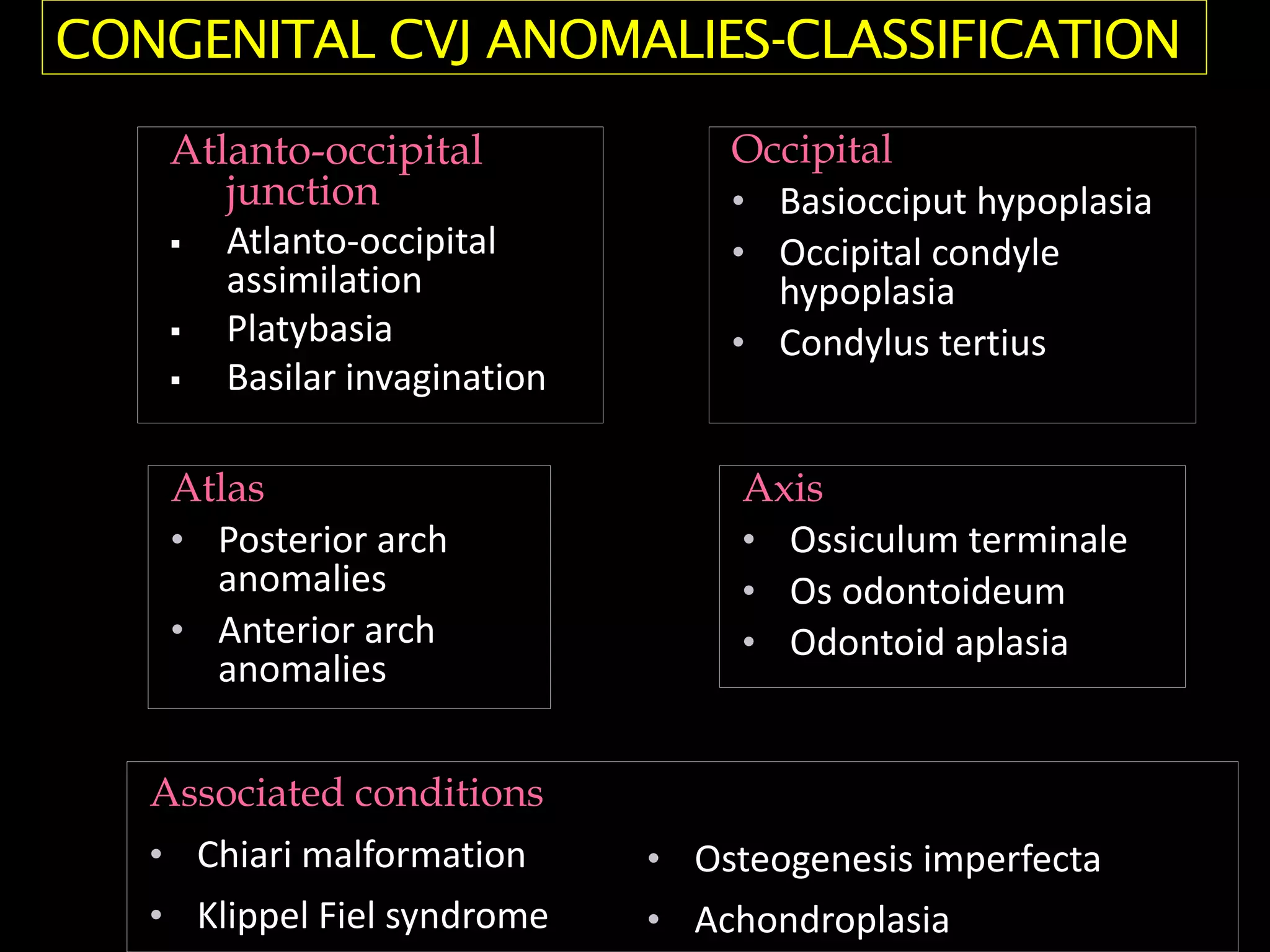
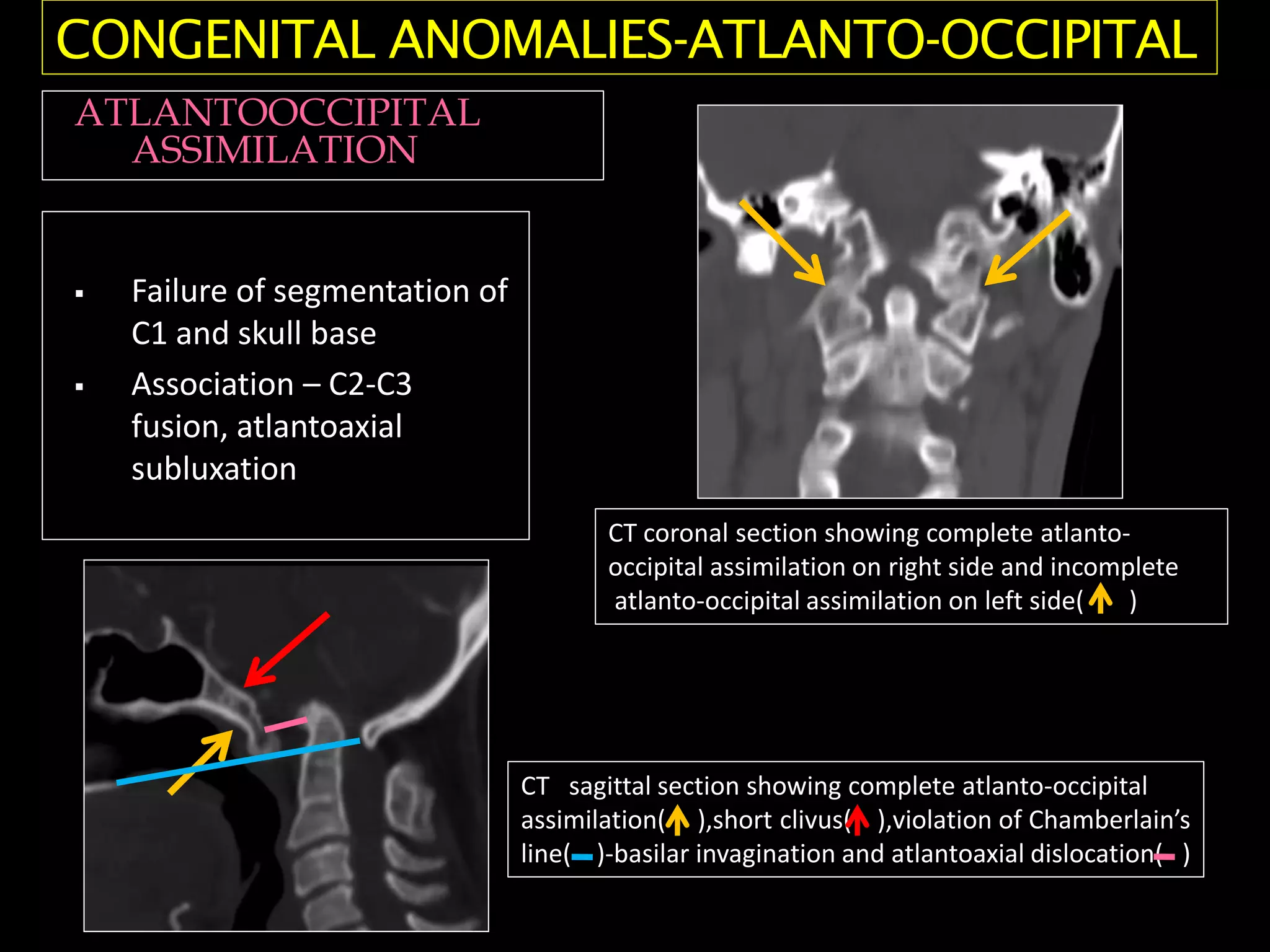
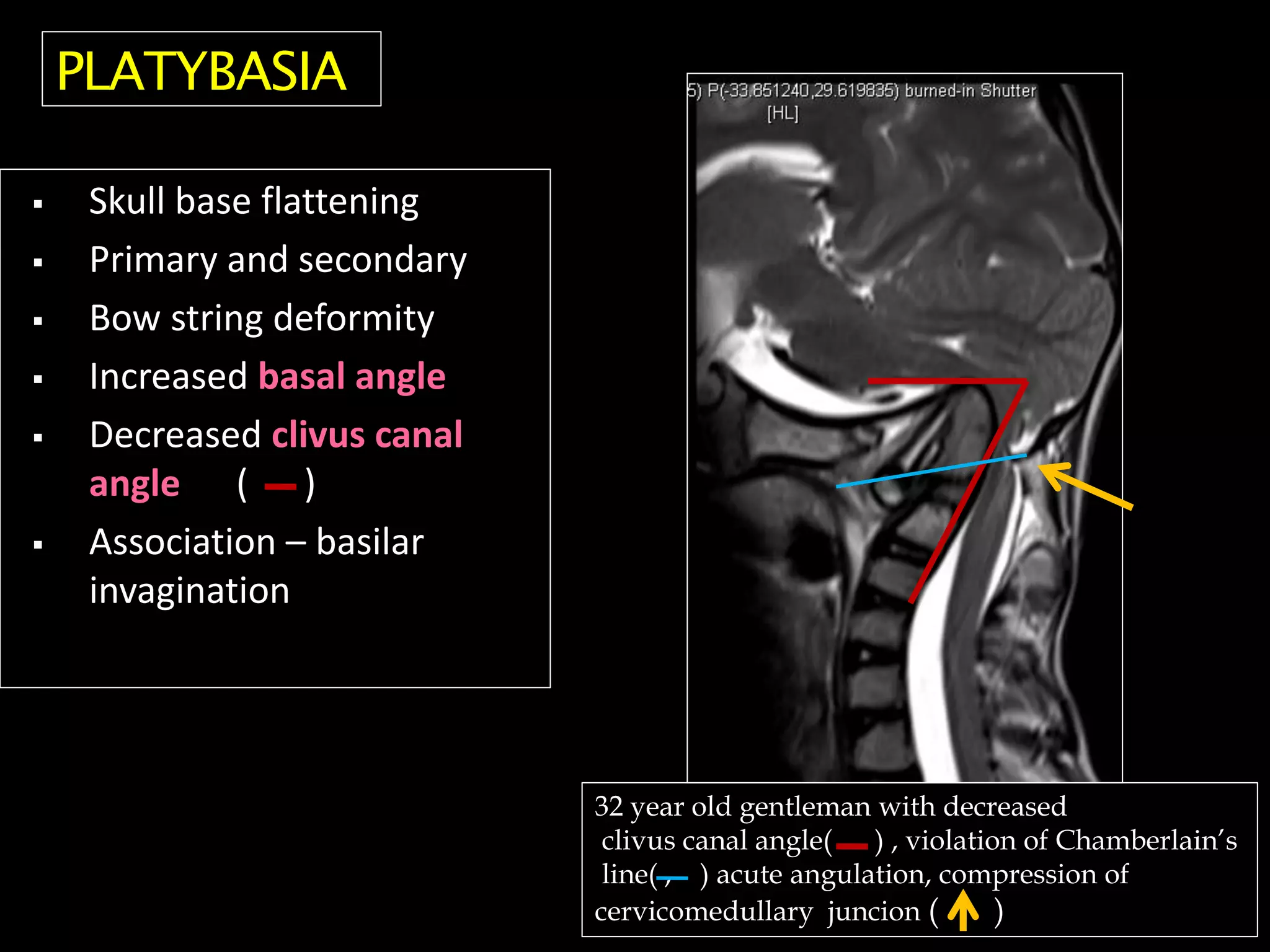
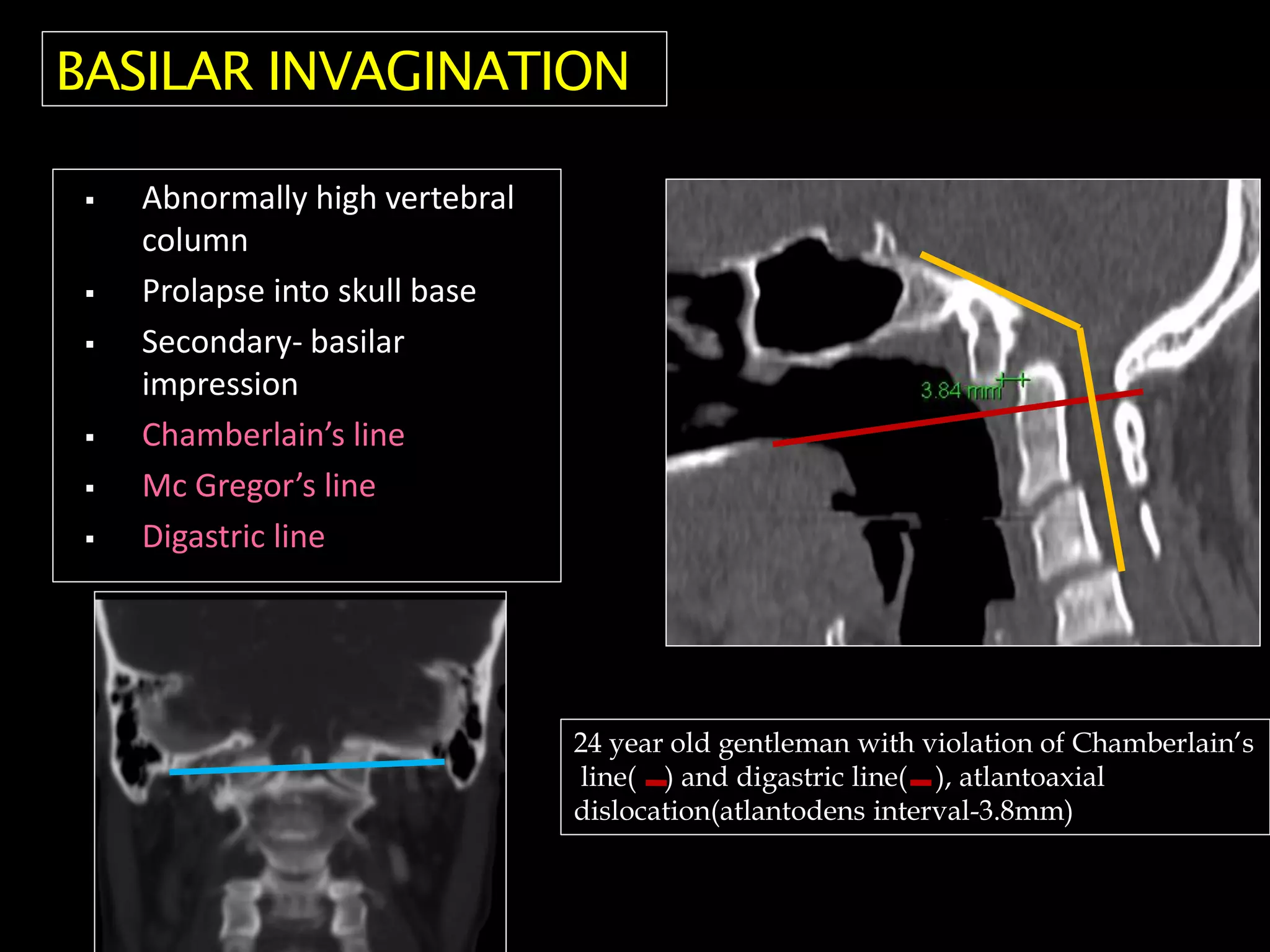
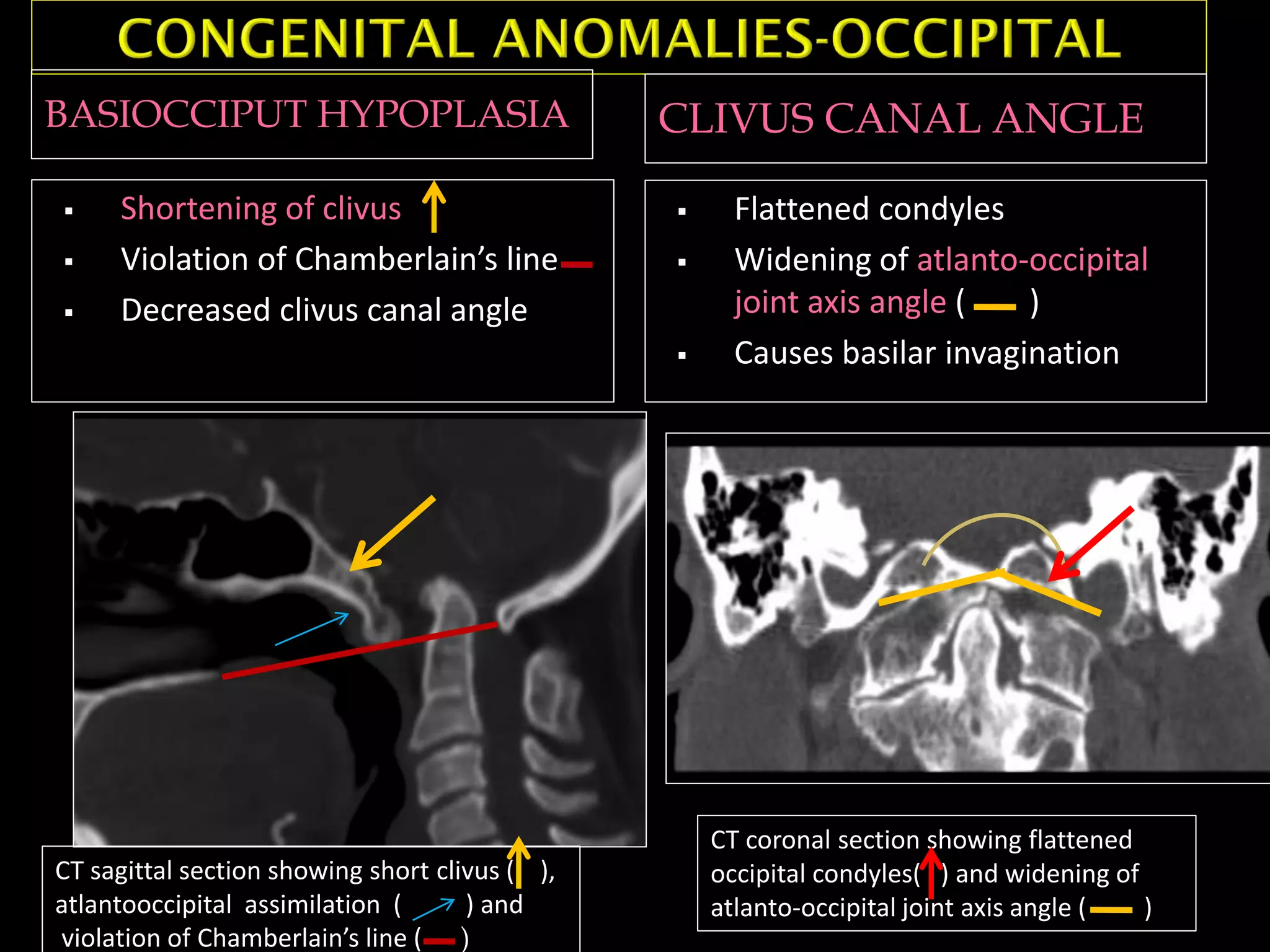
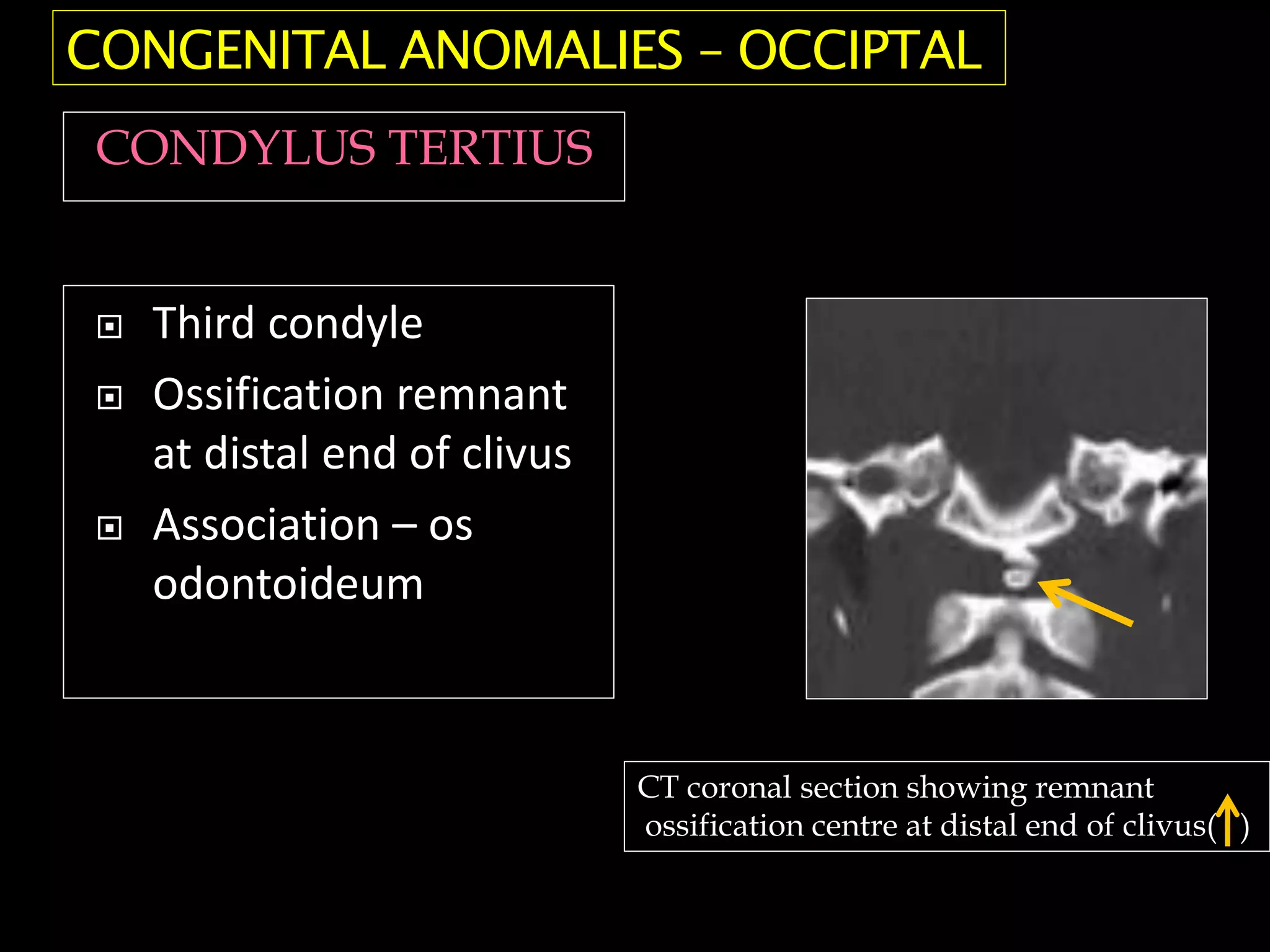
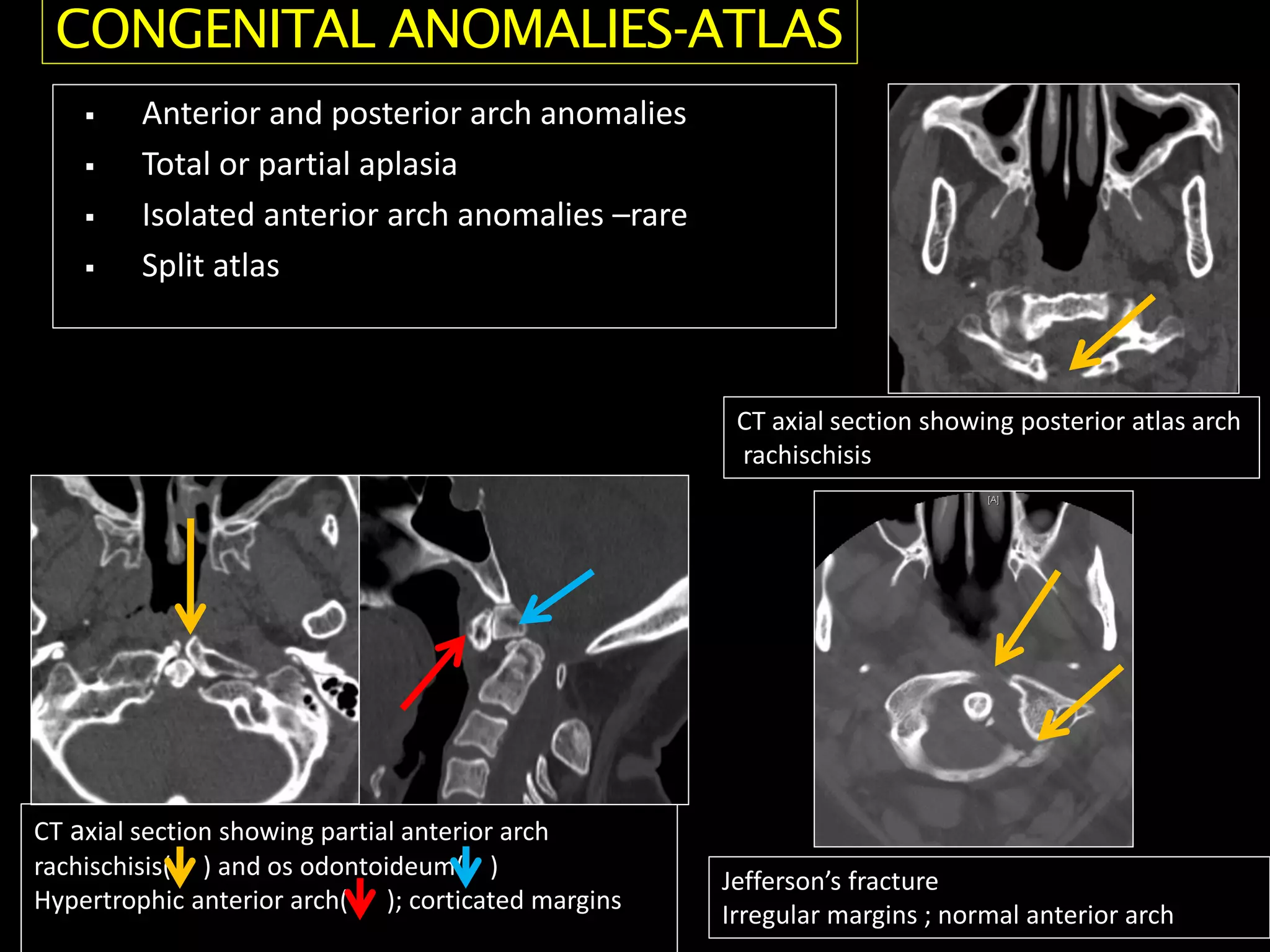
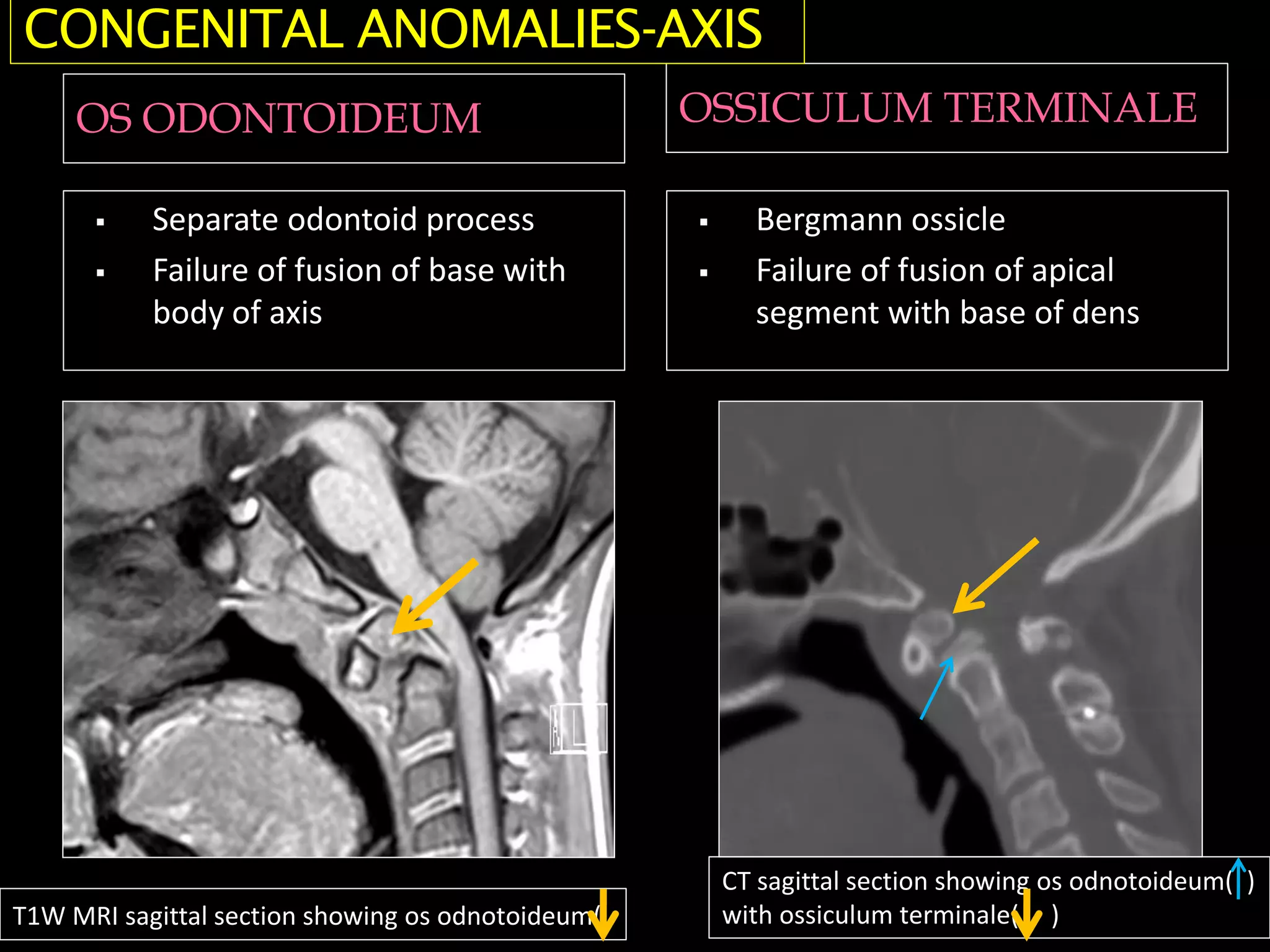
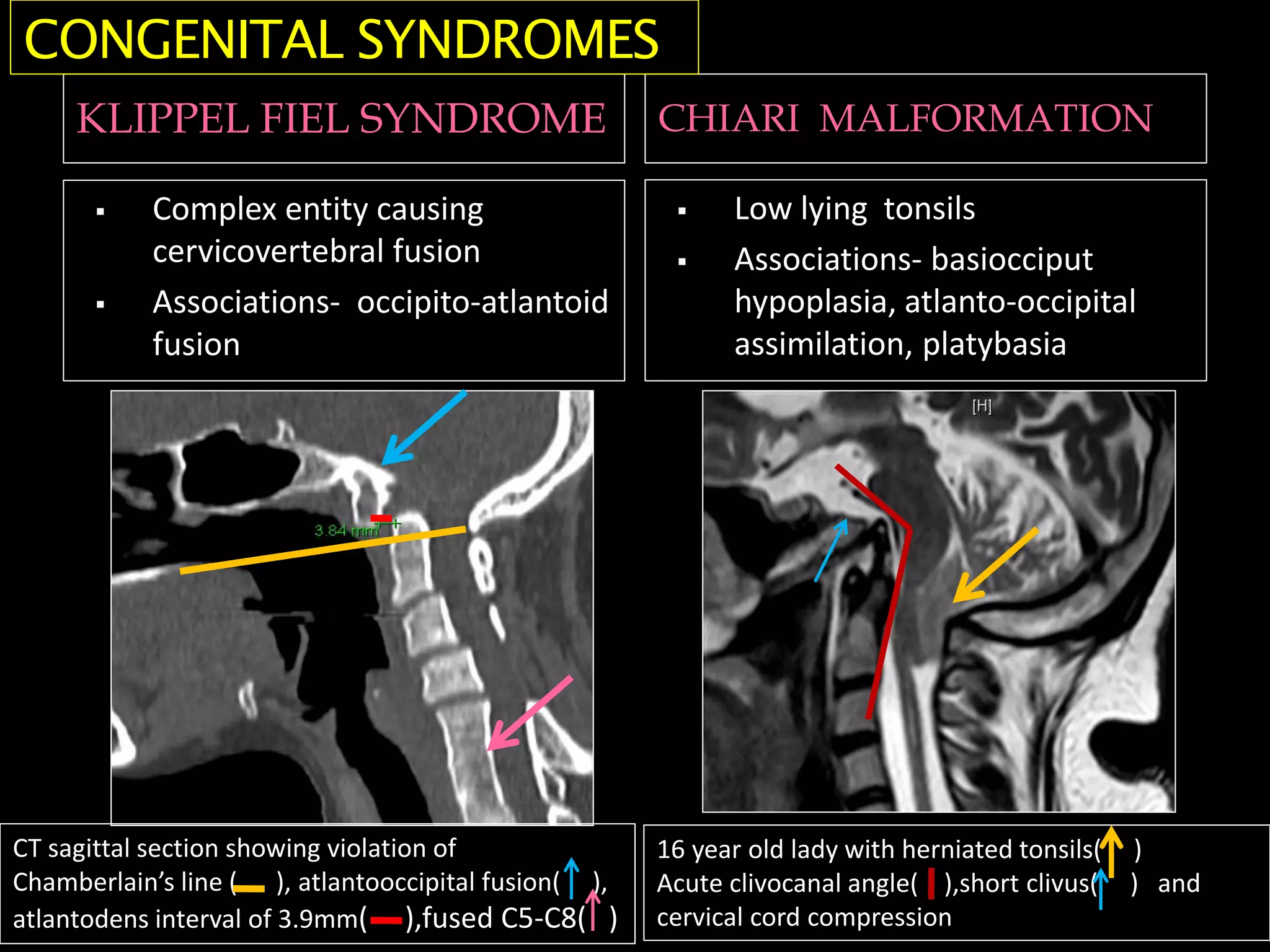
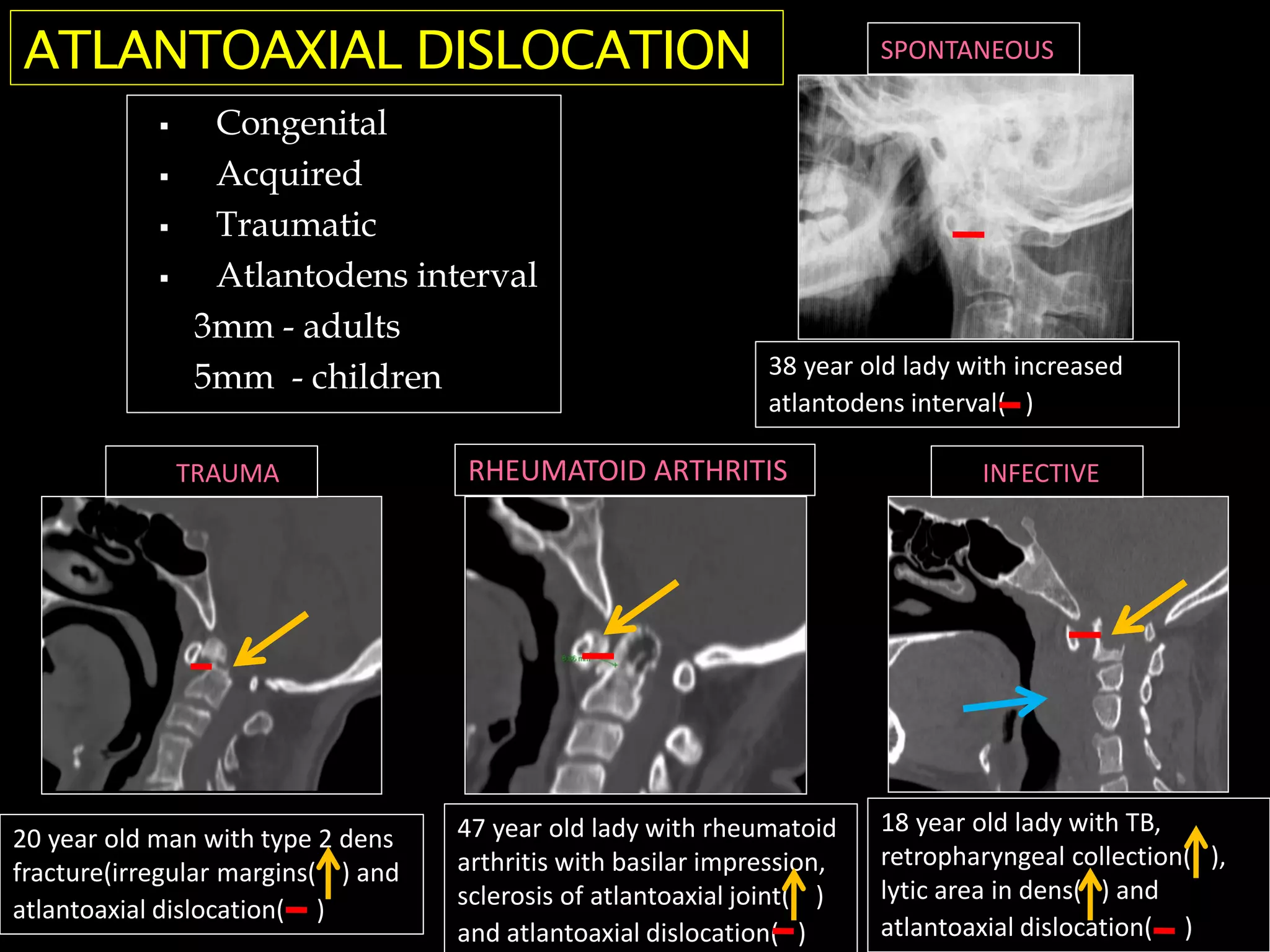
This document discusses various methods of craniometry used to diagnose craniovertebral junction (CVJ) anomalies through multimodality radiological assessment. It describes several important cranial landmarks and reference lines used to evaluate the CVJ, including Chamberlain's line, McRae's line, McGregor's line, and Wackenheim's line. It then classifies common congenital CVJ anomalies such as atlanto-occipital assimilation, platybasia, basilar invagination, occipital condyle hypoplasia, atlas anomalies, axis anomalies, and discusses associated conditions like Chiari malformation.