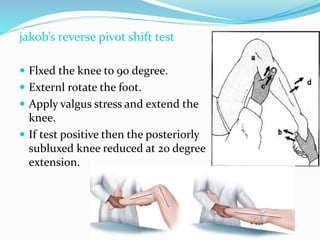
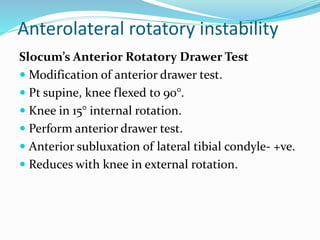
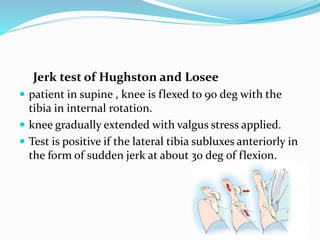
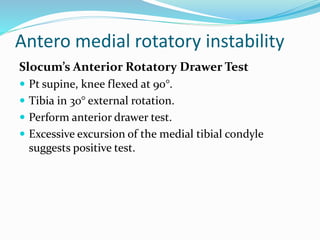
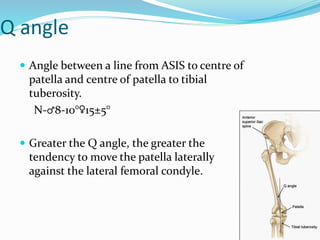
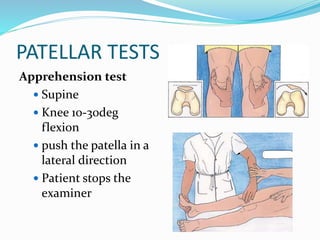
This document provides an overview of the anatomy and examination of the knee joint. It begins with the introduction and then describes the anatomy, including the osseous structures, tendons, ligaments, and intra-articular structures. It discusses taking a history and performing a routine examination, including inspection, palpation, range of motion tests, and special tests for injuries like meniscal tears and ligament injuries. The document provides detail on evaluating various symptoms, common injuries, and clinical tests to assess the knee.

































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





