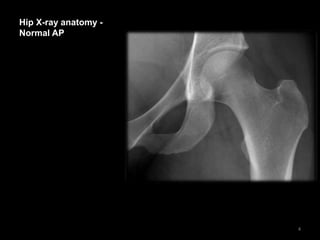
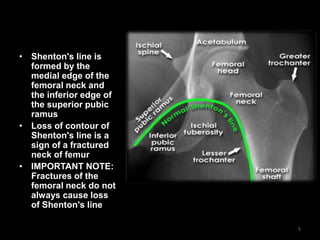
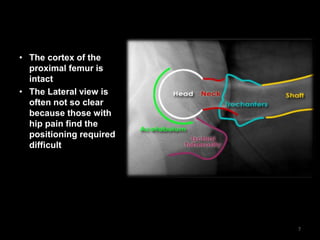
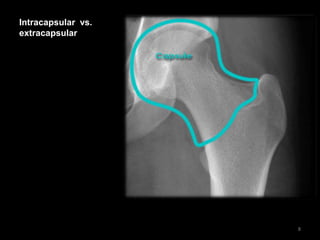
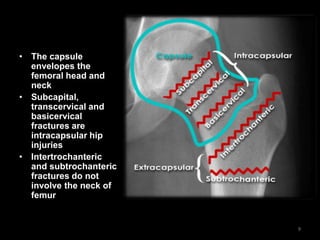
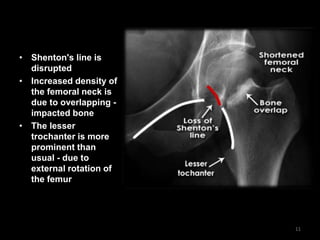
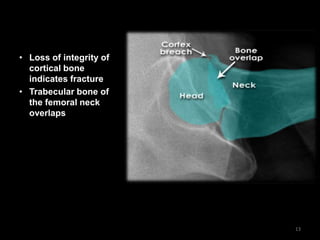
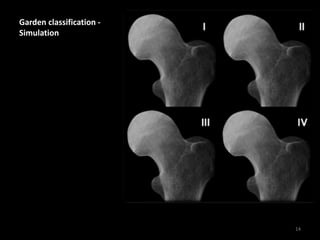
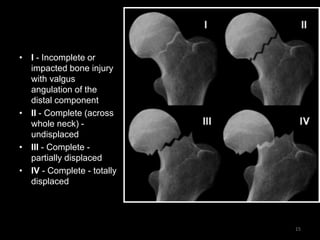
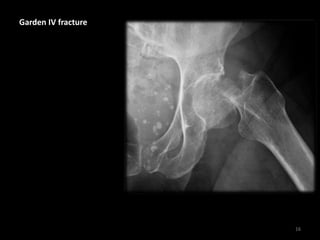
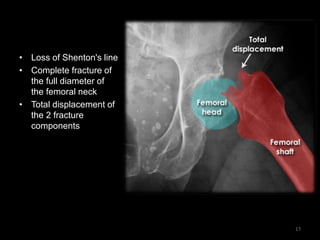
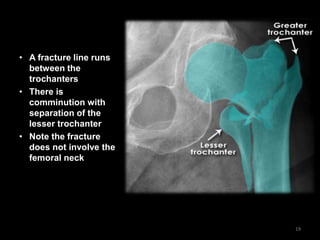
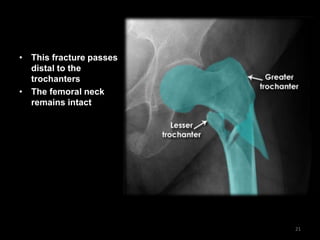
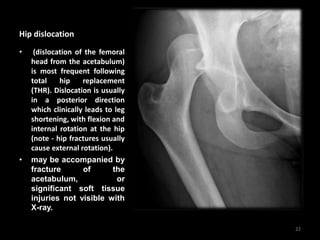
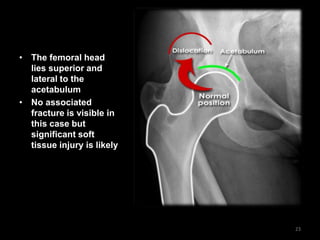
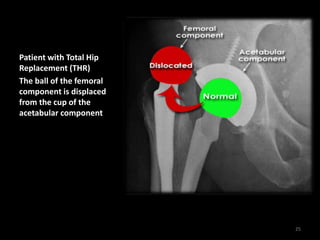
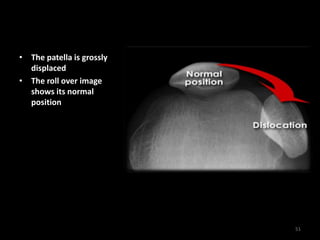
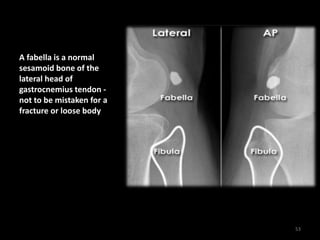
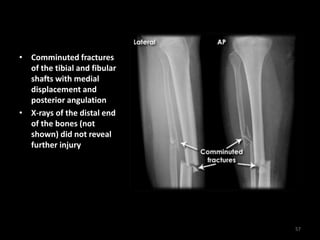
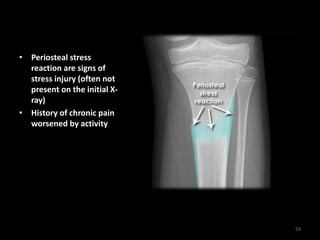
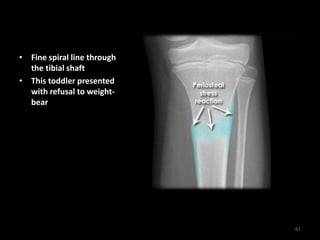
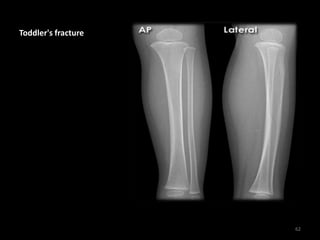
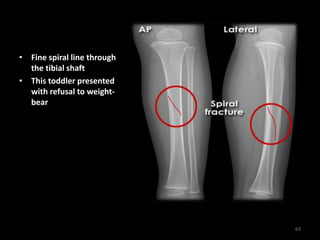
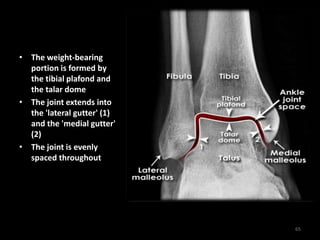
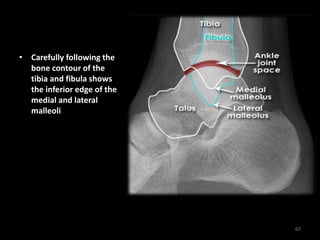
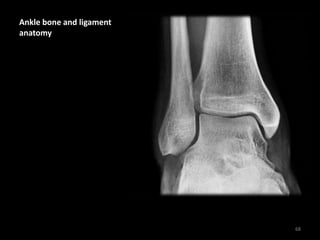
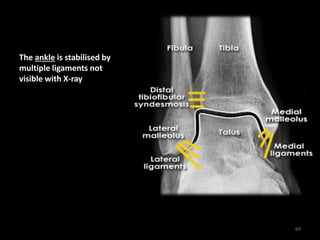
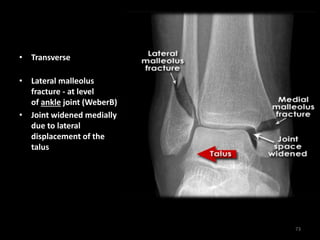
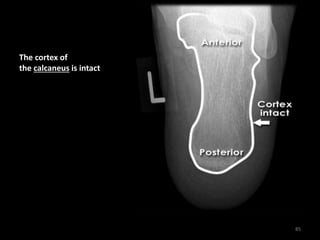
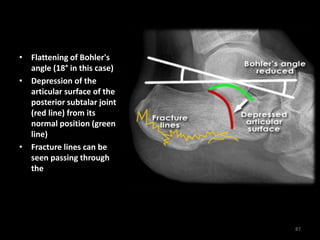
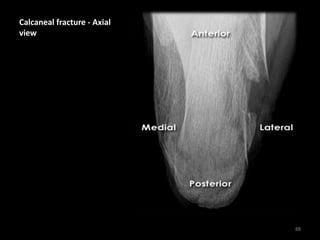
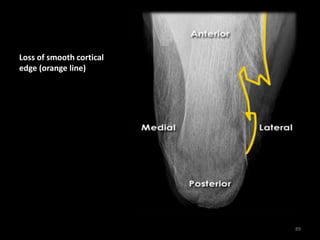
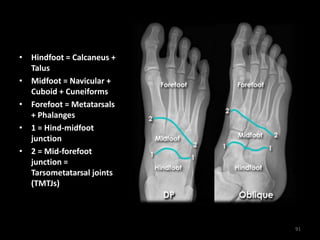
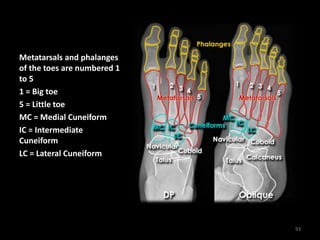
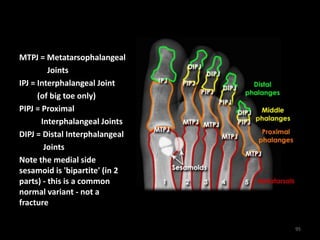
This document provides an overview of lower limb fractures seen on x-rays, including the pelvis, hip, femur, knee, ankle, and foot. It describes normal anatomy and examples of various fractures, such as femoral neck fractures, tibial plateau fractures, ankle fractures including trimalleolar fractures, and calcaneal fractures. Clinical information is provided for some cases. The document also discusses fracture classifications including Garden classification for femoral neck fractures.