Downloaded 807 times
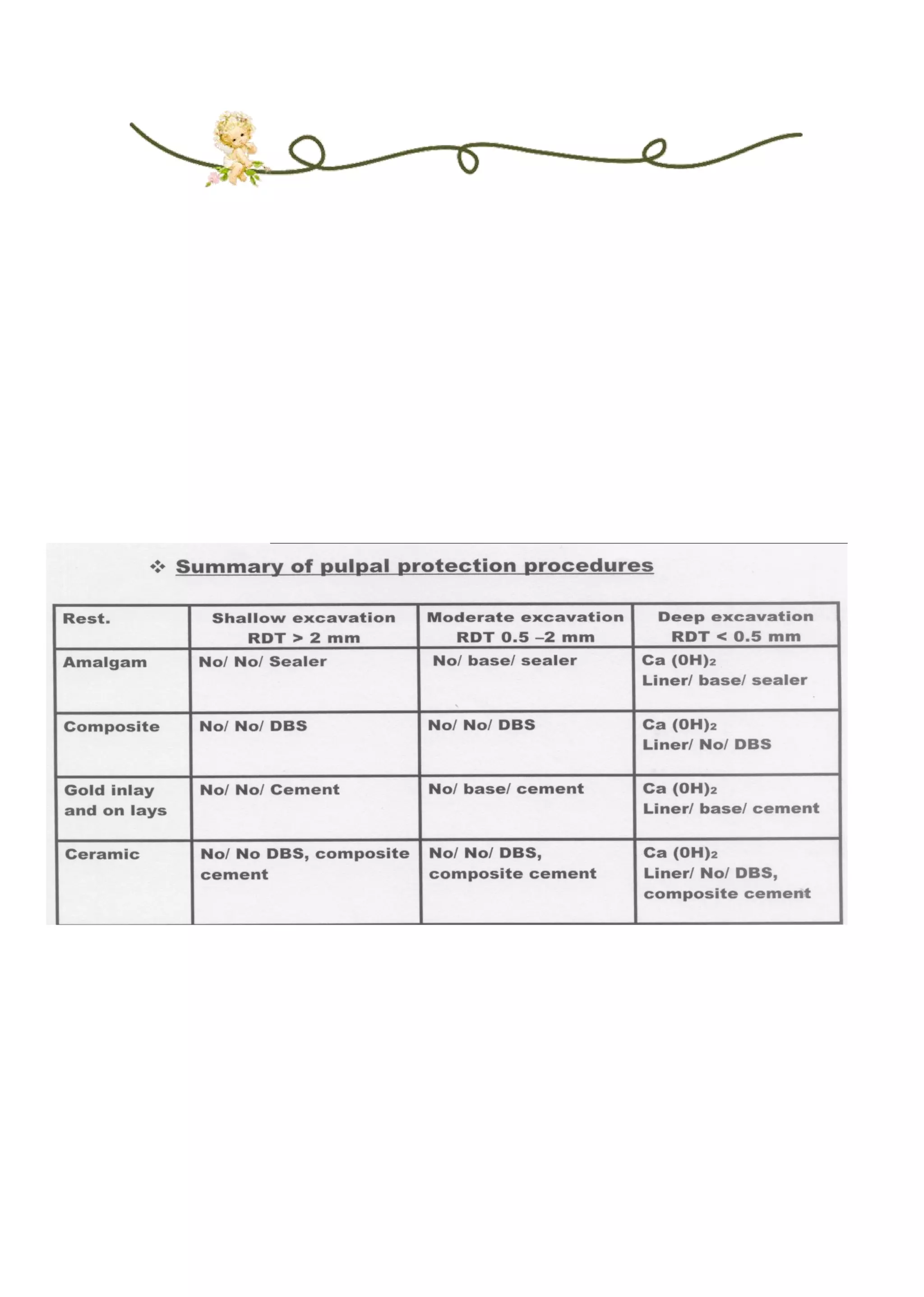
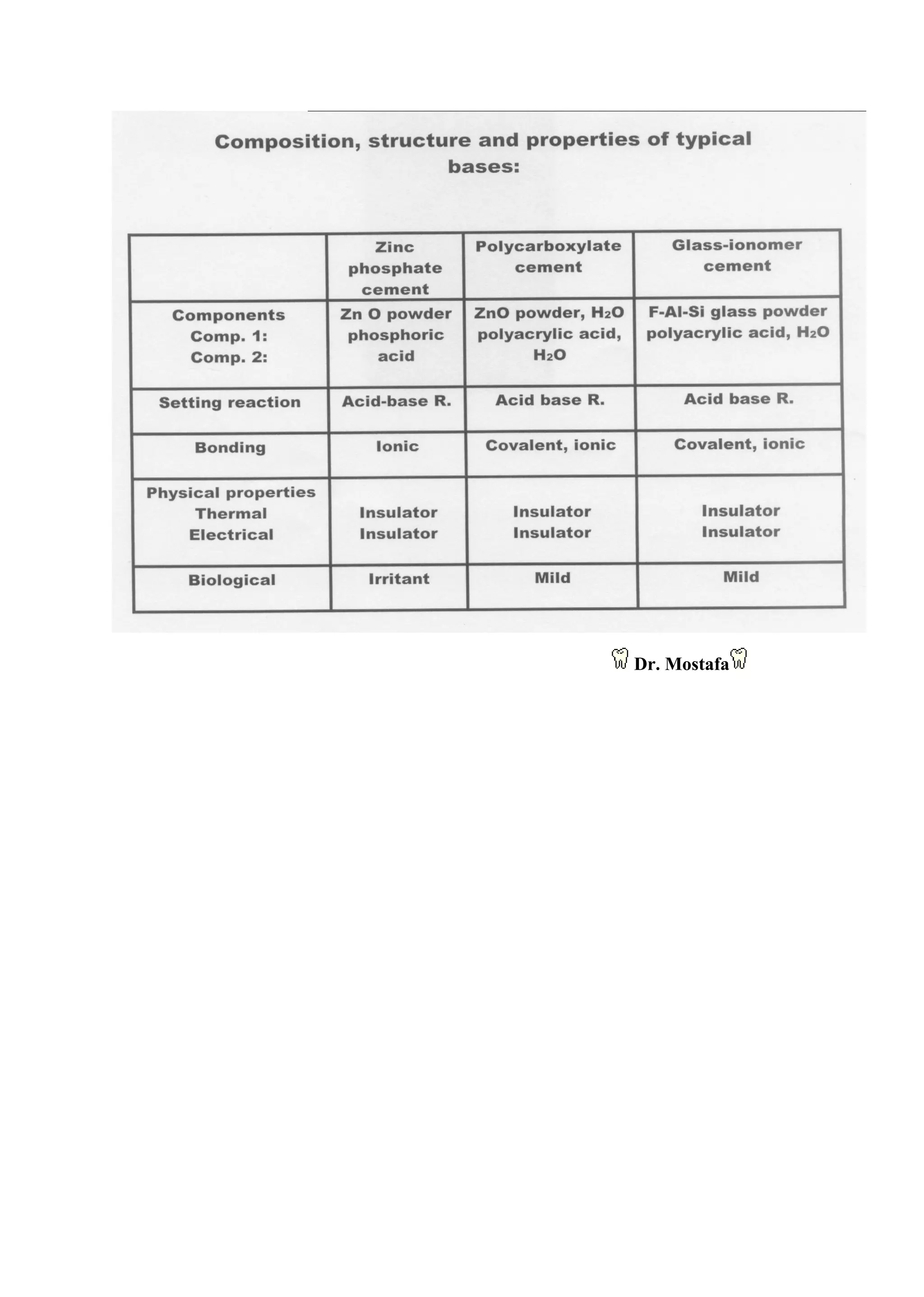
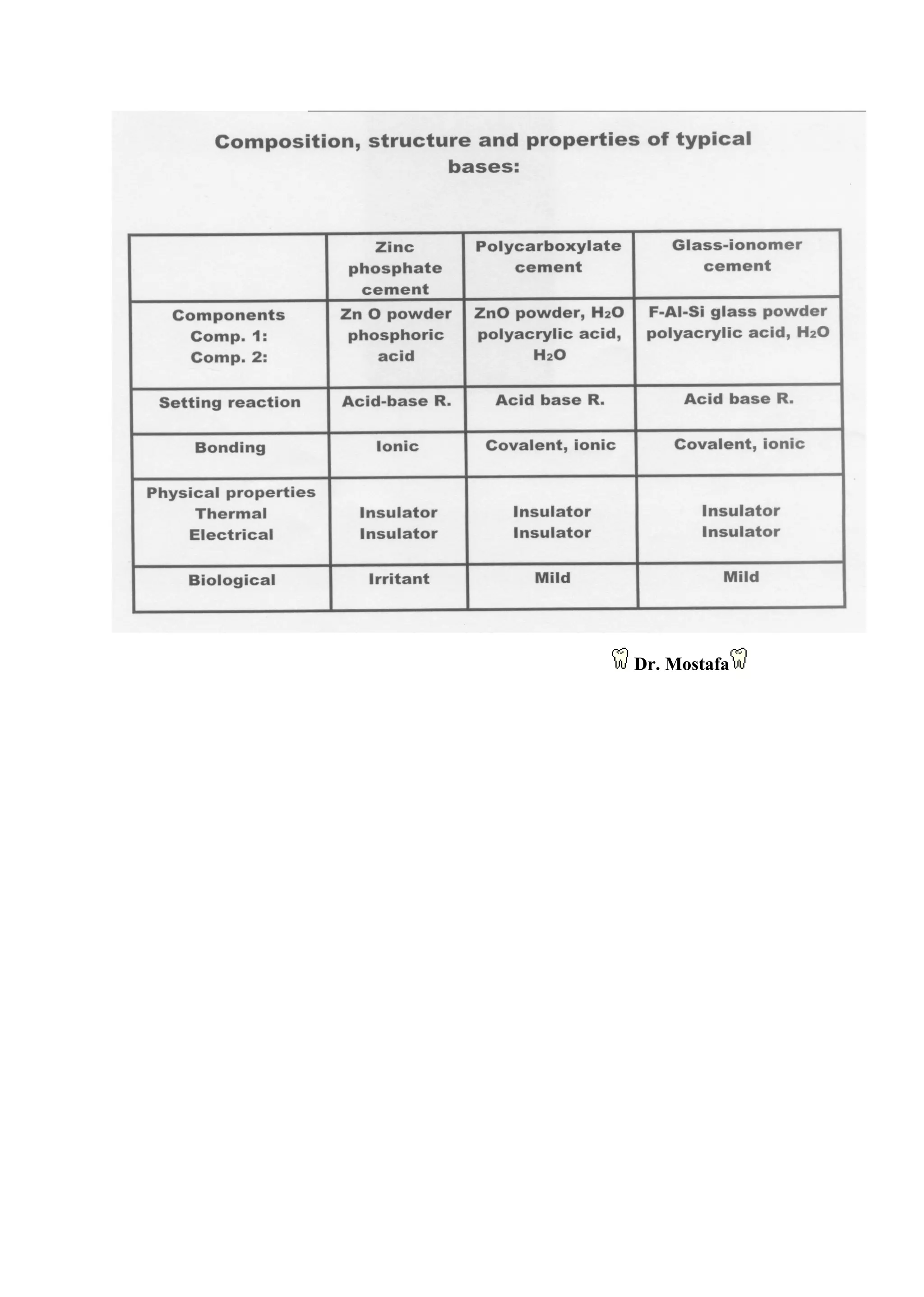

Liners and bases are placed between dentin (or pulp) and a restoration to provide pulpal protection. Liners are thin layers that provide a barrier against residual reactants and oral fluids penetrating between the restoration and tooth. Bases are thicker (1-2mm) and provide additional thermal protection and support restoration forces. The need for liners depends on the restoration material and cavity location/depth. Newer liners focus on chemical protection through sealing and adhesion rather than pulpal medication. The choice of liner depends on remaining dentin thickness and restoration material.









































































