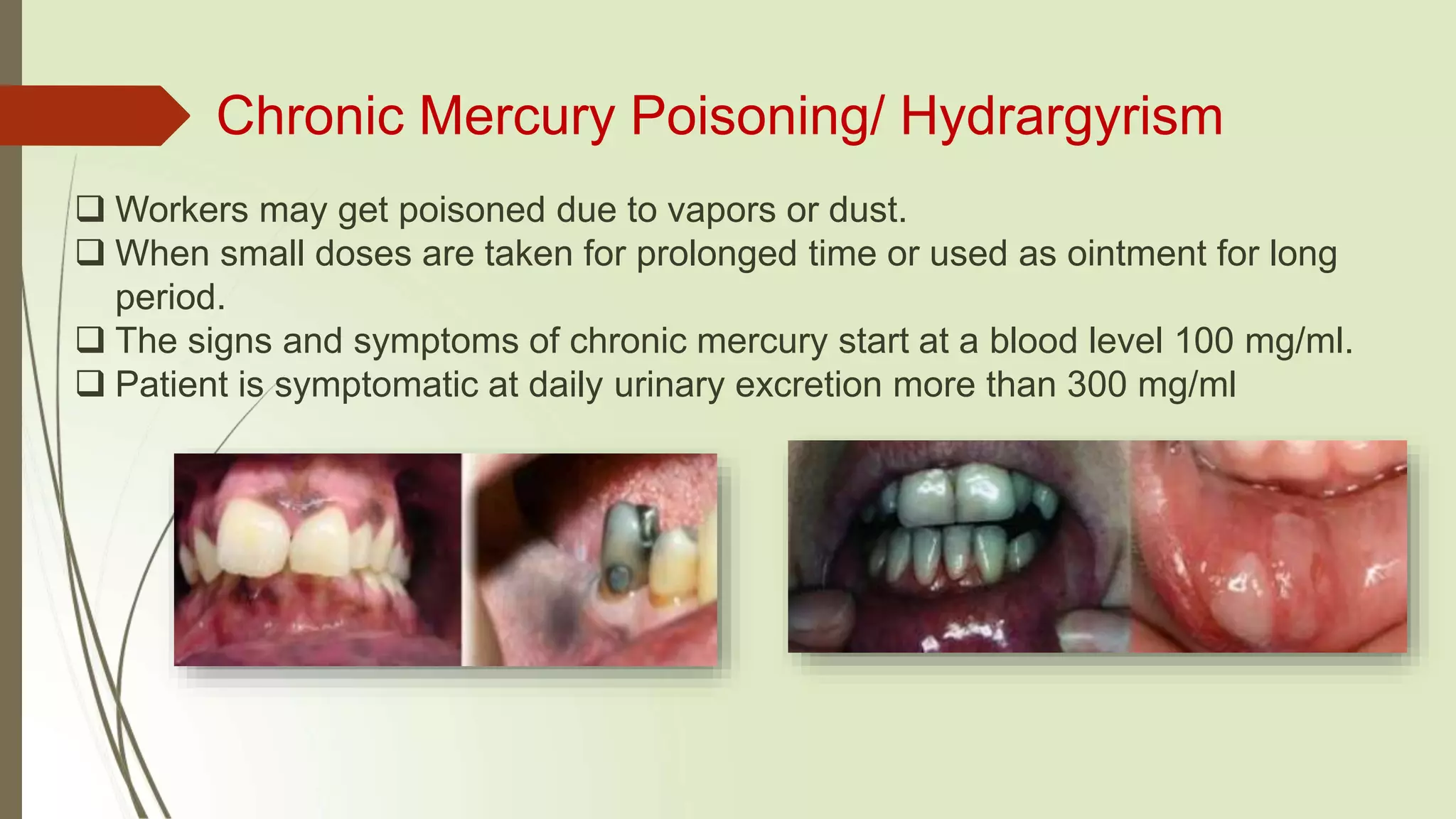
Mercury toxicity can occur from exposure to mercury in various forms. Elemental mercury is a liquid metal that vaporizes at room temperature into an odorless gas. Inorganic mercury combines with other elements to form salts, while organic mercury combines with carbon. Dental amalgam used in fillings contains mercury. Exposure risks include inhalation of vapors during placement or removal of fillings. Mercury is a potent neurotoxin that can cross the blood-brain barrier and cause neurological and developmental effects. Symptoms of toxicity depend on the level and route of exposure, ranging from rashes to kidney damage.