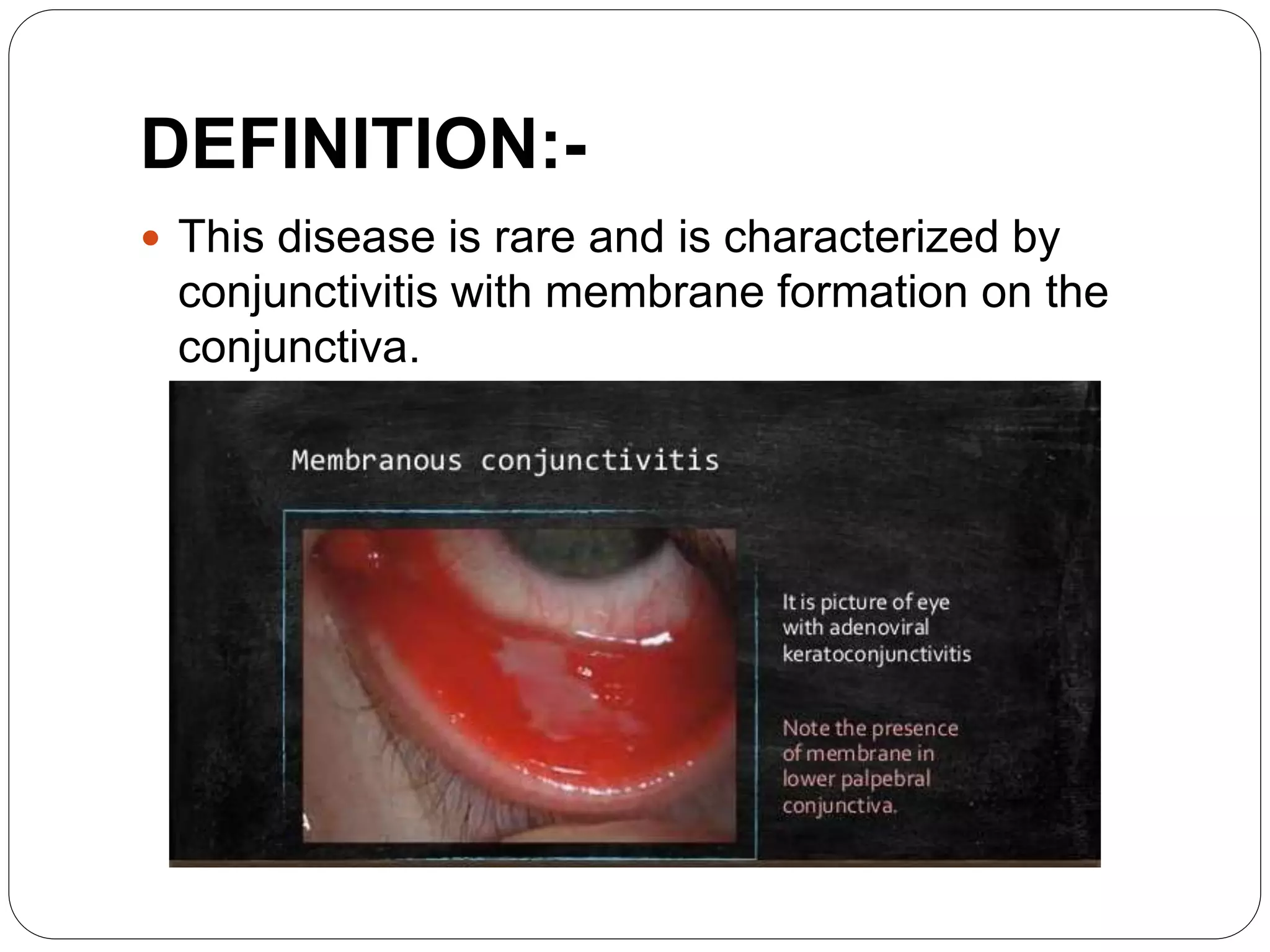
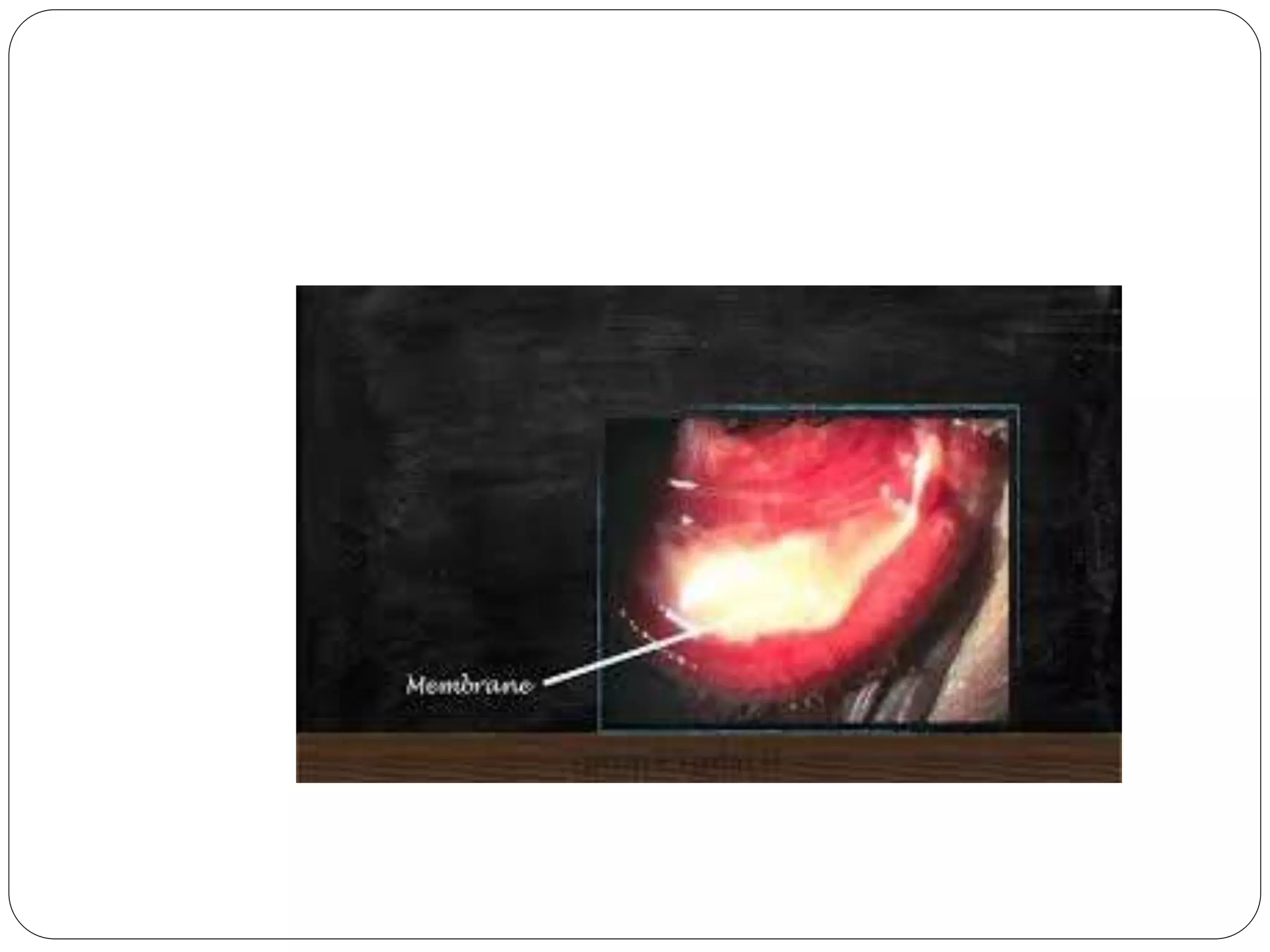
This document describes membranous conjunctivitis, a rare disease characterized by conjunctivitis and membrane formation on the conjunctiva. It most commonly affects children ages 2-8 and can be caused by bacteria like Corynebacterium diphtheriae. Symptoms include eyelid swelling, discharge, and pain. A white membrane will be seen on the eyelids. Treatment involves isolating the patient, administering anti-diphtheritic serum and antibiotics like penicillin both topically and systemically. Complications can include corneal ulcers or loss of the entire cornea if severe.