Medical Microbiology Laboratory (sample collection)
The document provides guidelines for collecting and transporting various medical specimens for microbiological laboratory testing. It discusses appropriate collection, labeling, and transport methods for common specimens including blood, urine, sputum, swabs, stool, pus, and cerebrospinal fluid. Proper collection and rapid transport of adequate and correctly labeled samples are essential for successful laboratory investigations and accurate patient diagnosis and treatment.
Medical Microbiology Laboratory (sample collection)
1.
Medical Microbiology Laboratory
(SampleCollection)
Hussein A. Abid
Medical Laboratory Scientist
Member at American Society of Microbiology
Chairman of Iraqi Medical Laboratory Association
Teacher at Middle Technical University
2.
2
SUCCESSFUL LABORATORY INVESTIGATIONS
Collection of adequate and appropriate specimens.
Sufficient documentation.
Biosafety and decontamination.
Correct packaging and rapid transport (e.g., sample
to be send out for TB culture).
Timely communication of results.
4
SPECIMEN COLLECTION (NOTES)
Must be collected correctly:
If not, may not grow in culture
Contaminants may be mistakenly
identified
Patient may receive incorrect or
harmful therapy
5.
5
SPECIMEN COLLECTION (GUIDELINES)
Avoid causing harm or
discomfort to patient
Collect from appropriate site
Obtain specimen at correct
time
Use appropriate devices
Obtain sufficient quantity
of specimen
Obtain specimen prior to
the start of antimicrobial
therapy
Label correctly
7
WHAT CONTAINERS TOUSE?
Containers must be leak proof
Unbreakable
For cultures sterile containers a Must
8.
8
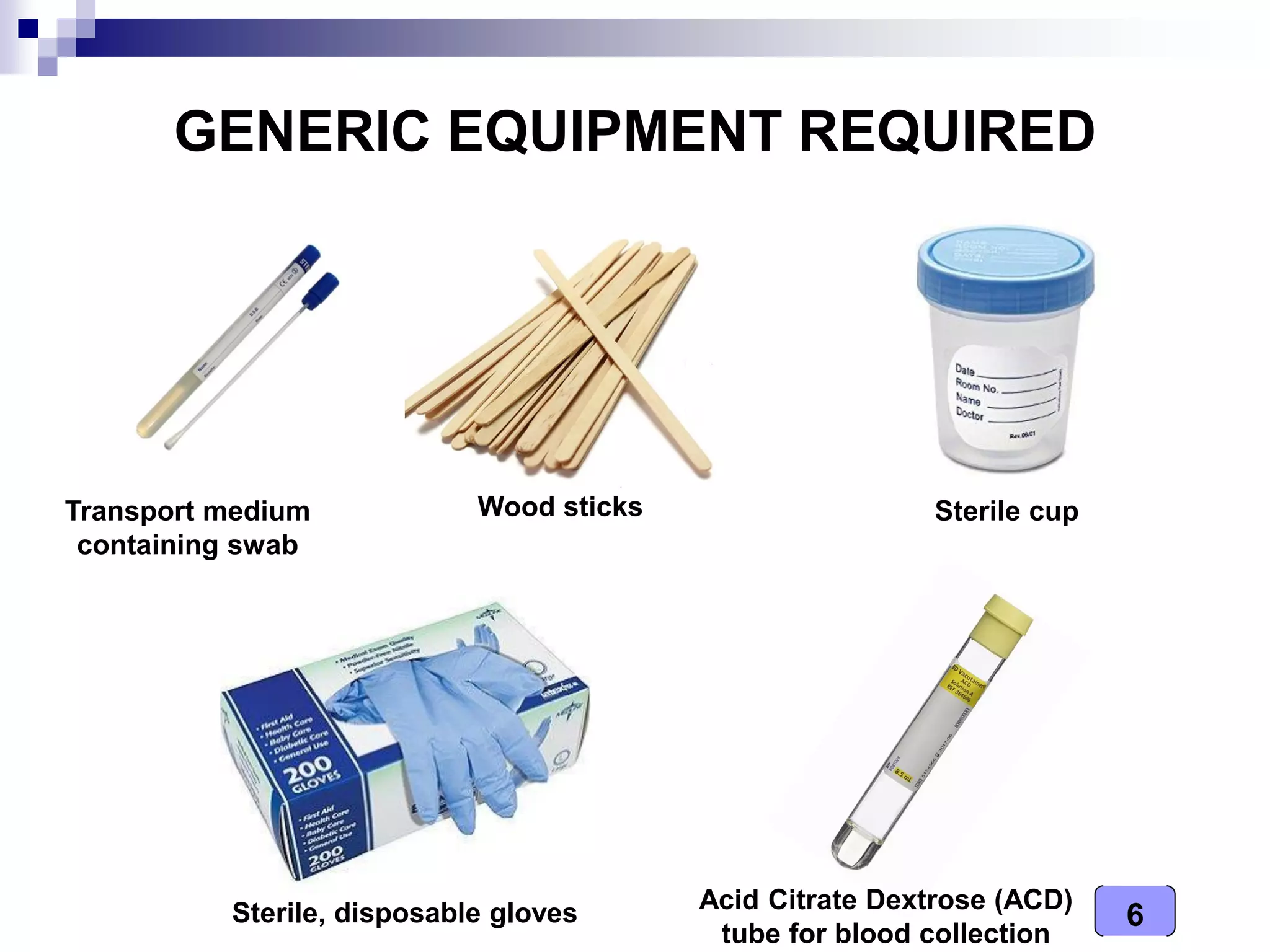
SPECIMEN COLLECTION
Devices
oUse appropriate collection
device or specimen container
o Sterile swabs – absorbent
material on the tip
Collection and transporting systems
o Sterile, self-contained
o Transport medium
o Aerobic or anaerobic
9.
9
TRANSPORT MEDIUM
Transportmedium is a safe and an appropriate way of
carrying the clinical specimens from distances (long or
short) for transporting to the lab for examination.
o It allows organisms to survive.
o It does not allow organisms to proliferate.
Examples:
o For bacteria – Cary Blair
o For viruses – virus transport media (VTM)
10.
10
1. BLOOD COLLECTION(for culture)
Venous blood (during high peak fever):
infants: 0.5 – 2 ml
children: 2 – 5 ml
adults: 5 – 10 ml
11.
11
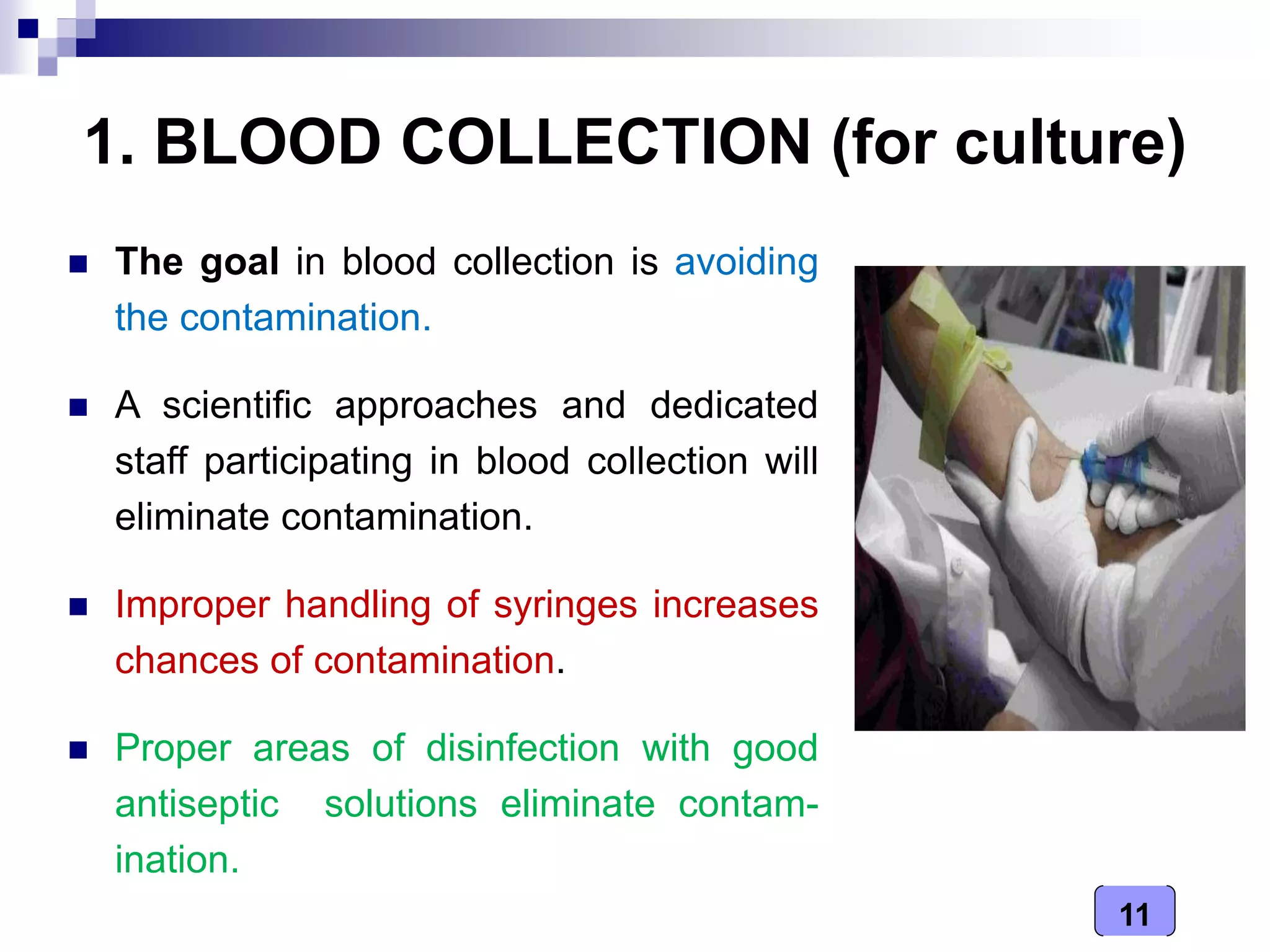
1. BLOOD COLLECTION(for culture)
The goal in blood collection is avoiding
the contamination.
A scientific approaches and dedicated
staff participating in blood collection will
eliminate contamination.
Improper handling of syringes increases
chances of contamination.
Proper areas of disinfection with good
antiseptic solutions eliminate contam-
ination.
12.
12
1. BLOOD COLLECTION(for culture)
Handling and transport
Collect into blood culture bottles
(broth)
Request slip must contain relevant
patient information
Send immediately to laboratory
with request slip
Blood culture bottles
13.
13
2. URINE
Specimen:
Earlymorning midstream urine is
obtained aseptically.
From babies, urine is collected in
sterile plastic bags.
Transport:
Transport to laboratory within one hour or
kept at 4 ºC to avoid multiplication of bacteria in urine.
14.
14
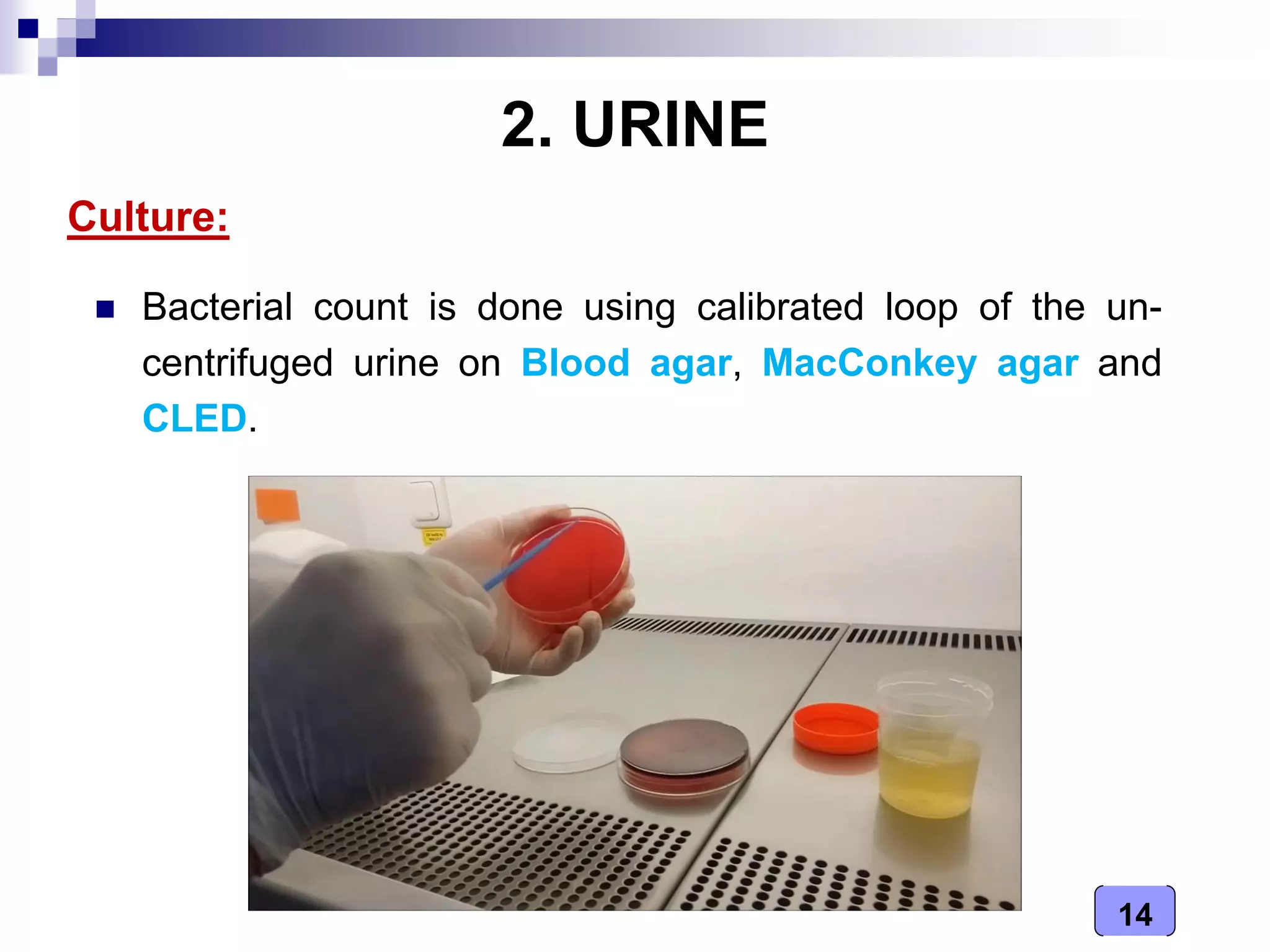
2. URINE
Culture:
Bacterialcount is done using calibrated loop of the un-
centrifuged urine on Blood agar, MacConkey agar and
CLED.
15.
15
3. SPUTUM
Collection ofspecimen:
Patient is instructed to take a deep
breath and cough up sputum
directly into a wide-mouth sterile
container of 50-100 ml capacity.
Avoid saliva or postnasal disch-
arge.
Minimum volume 1 ml.
16.
16
4. SWABS
Aplain cotton wool swab
should be used to collect as
much exudates as possible
from tonsils, posterior
pharyngeal wall and other
area that is inflamed or
bears exudates.
a) Throat swab (posterior pharyngeal swab)
17.
17
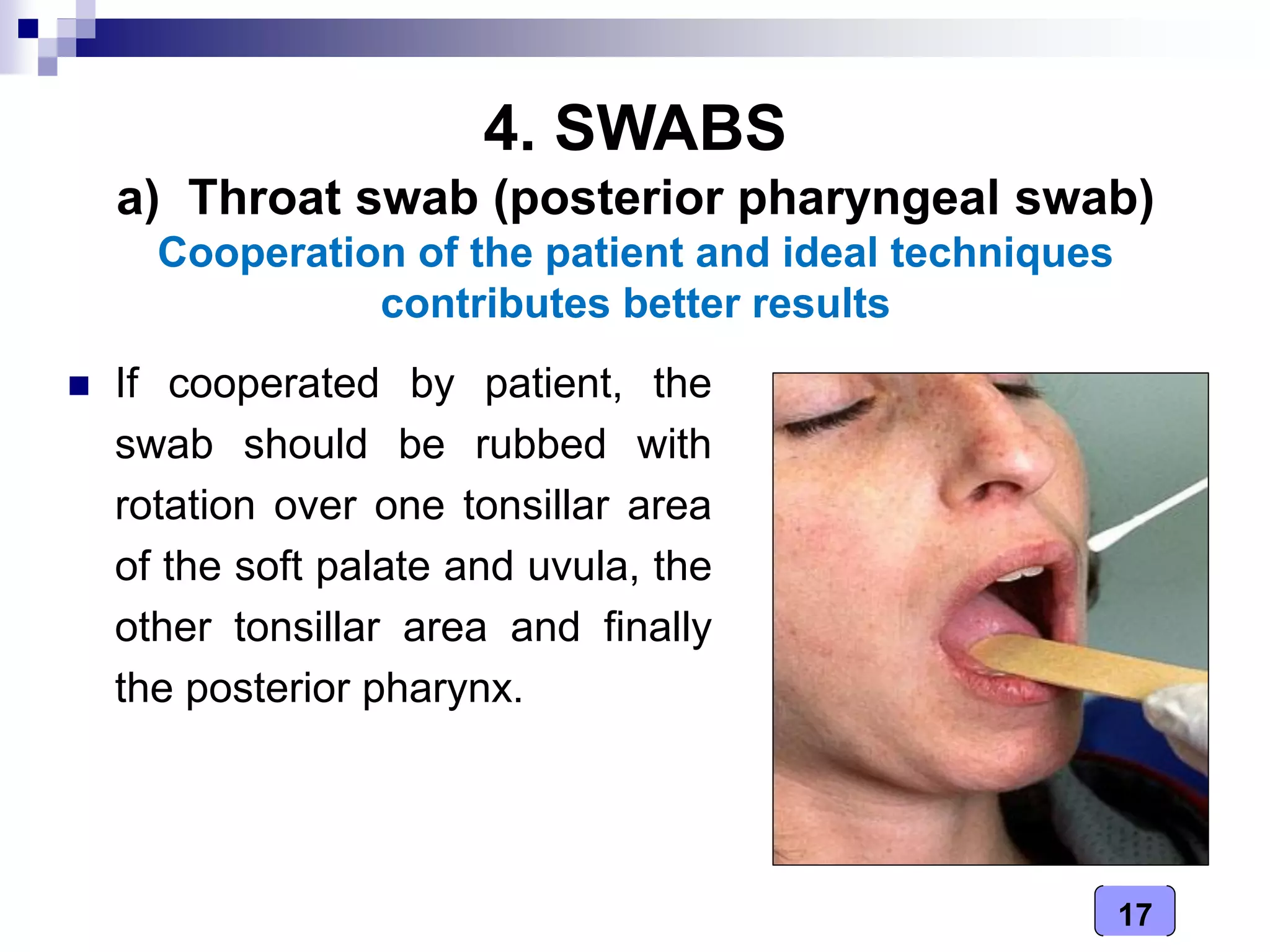
4. SWABS
Ifcooperated by patient, the
swab should be rubbed with
rotation over one tonsillar area
of the soft palate and uvula, the
other tonsillar area and finally
the posterior pharynx.
a) Throat swab (posterior pharyngeal swab)
Cooperation of the patient and ideal techniques
contributes better results
18.
18
4. SWABS
Tilthead backwards
Insert flexible fine-shafted
polyester swab into nostril
and back to nasopharynx
Leave in place a few seconds
Withdraw slowly; rotating motion
b) Nasopharyngeal swab
19.
19
4. SWABS
Nodrops should have been
used 3 hours prior to taking
the swab.
Place the swab into the outer
ear and rotate gently once.
c) Ear swab
20.
20
4. SWABS
Itis ideal to pick up the
material with the thin
serum coated swab.
Clinical material from
Conjunctiva, i.e. from
averted eyelid
The margin of the eyelid
should be avoided.
d) Eye swab
21.
21
4. SWABS
Aftercareful cleaning of the
wound site, a swab was taken
from the inner side of the wound
or the area where pus is
accumulated.
Rotate the swab gently once.
e) Pus swab (from wounds)
22.
22
5. STOOL SAMPLES
Whenever possible, a specimen
of stool should be collected.
A rectal swab is unsatisfactory,
unless it is heavily charged and
visibly stained with faeces
collected from rectum, not anus
23.
23
5. STOOL SAMPLES
Collectionand transportation
Freshly passed stool samples should be collected in
sterile container.
Avoid specimens from a bed pan.
Transmit the container quickly to laboratory.
If delay is unavoidable and particularly when the weather
is warm collect the specimens in a container holding
6 ml buffered glycerol saline transport medium.
24.
24
RECTAL SWABS
Advantages
convenient
Used for small children, debilitated patients and other
situations where voided stool sample not feasible
Drawbacks
no macroscopic assessment possible
less material available
not recommended for viruses
25.
25
6. PUS SAMPLES
Aspirate from abscess or wound in a sterile container.
Pus should always be aspirated, if possible, rather than
collecting a wound swab.
Should be transported immediately to the laboratory.
26.
26
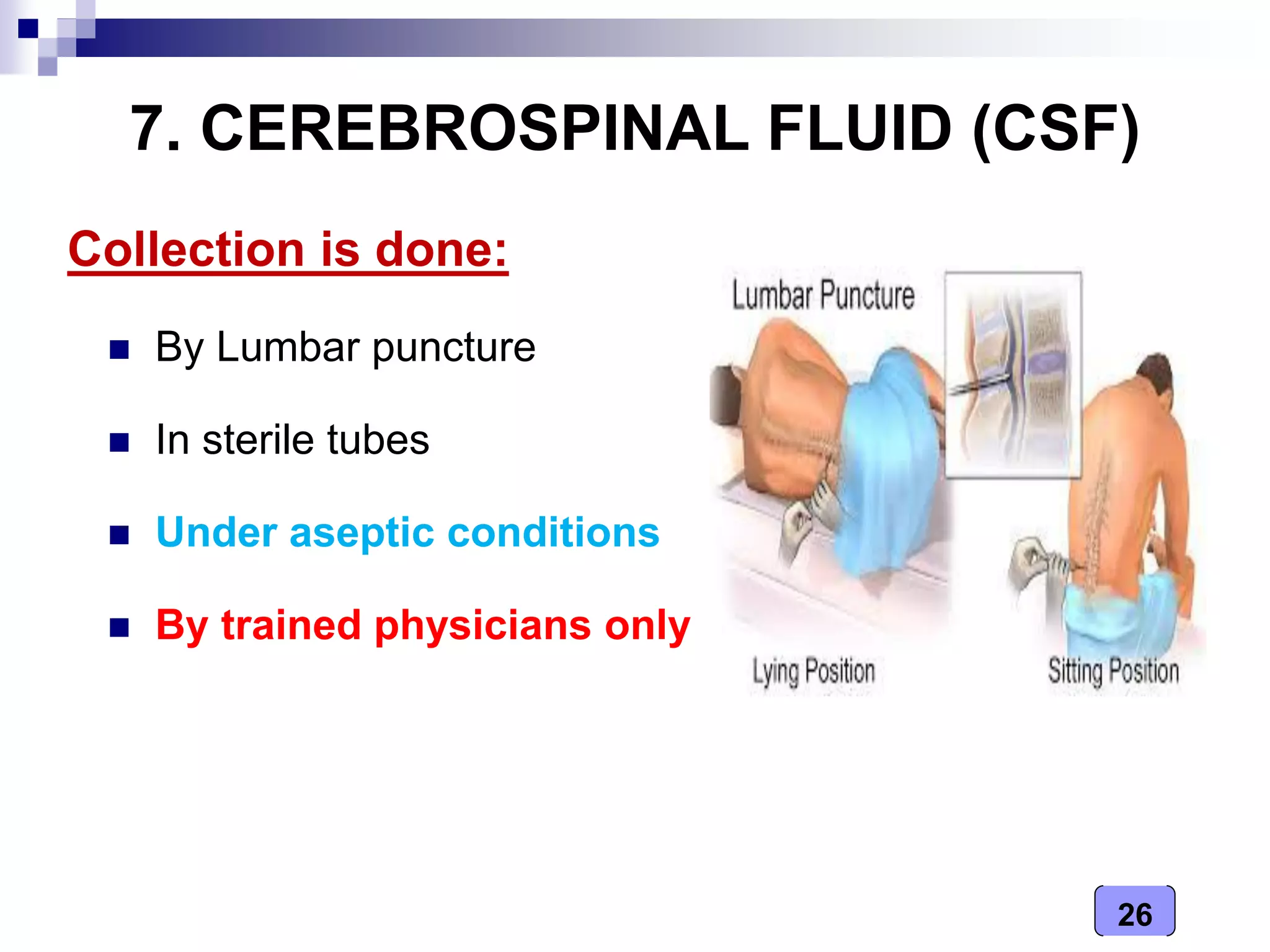
7. CEREBROSPINAL FLUID(CSF)
Collection is done:
By Lumbar puncture
In sterile tubes
Under aseptic conditions
By trained physicians only
27.
27
CSF NEEDS ANEW AND STERILE CONTAINER
Fresh sterile screw capped
container to be used.
Reused containers, not to
be used, contamination from
the previous specimens
misrepresent the present
specimen.
28.
28
TRANSPORTATION TO LABORATORY
The collected specimen of CSF to
be dispatched promptly to
Laboratory, delay may cause death
of delicate pathogens,
e.g., Meningococci and disintegrate
the leukocytes
29.
29
PRESERVATION OF CSF
It is important when there is
delay in transportation of
specimens to Laboratory
DO NOT keep in refrigerator,
which tends to kill H.
influenza
If delay is anticipated leave
at room temperature.