Downloaded 252 times

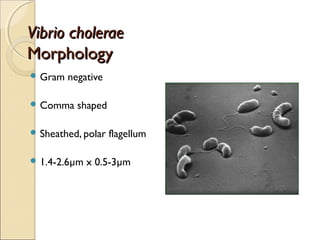


Vibrio cholerae is the bacterium that causes cholera. It is a comma-shaped, gram-negative bacterium that secretes a toxin causing massive diarrhea and dehydration. Cholera spreads through contaminated food and water and has caused several pandemics throughout history. The bacterium was first discovered by Filippo Pacini in 1854 and later rediscovered by Robert Koch in 1884. Symptoms of cholera include sudden onset of watery diarrhea and vomiting which can lead to severe dehydration and death if untreated.
















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













