Downloaded 14 times




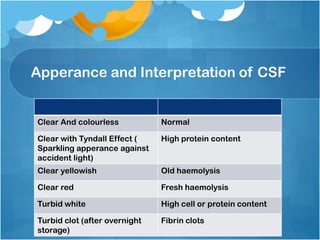



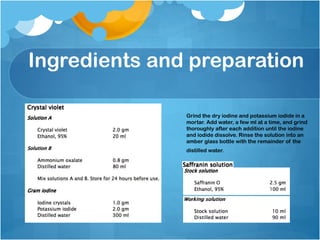
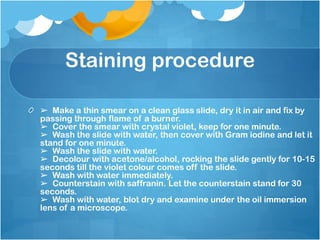
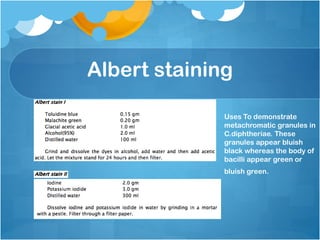
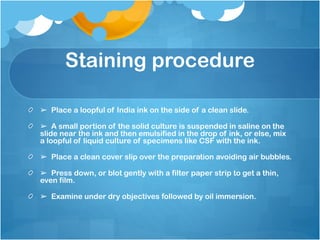
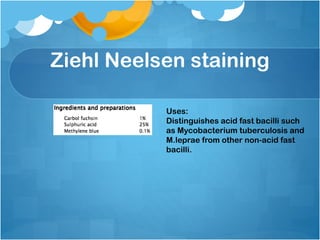
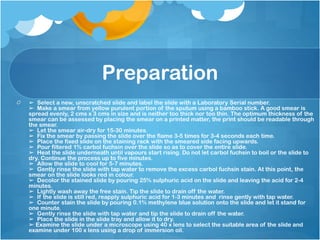
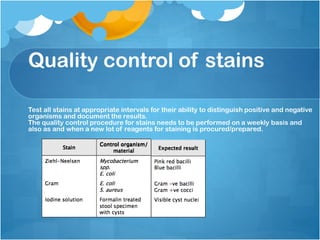

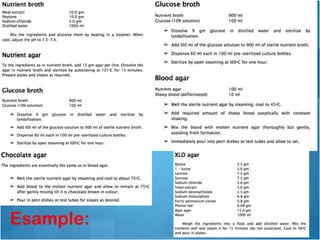



This document provides guidelines on standard operating procedures for microbiology laboratory diagnosis. It discusses the proper collection, transport, and processing of various clinical specimens like blood, cerebrospinal fluid, sputum, urine, stool, and others. Key points emphasized include collecting specimens before antimicrobial administration, using appropriate containers, minimizing delays in transport and storage, and preventing contamination. The document also outlines procedures for staining techniques, sterilization, waste disposal, and quality control. Following standardized protocols helps ensure accurate laboratory diagnosis of infectious diseases.

































































