

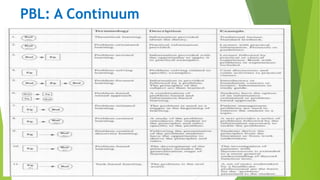

The document discusses various teaching methods used in medical education, including lectures, small group learning, problem/case-based learning, e-learning/computer-assisted instruction, self-instruction modules, and experiential learning through site visits and rotations. For each method, the document outlines strengths, weaknesses, and applications. It provides examples of how different methods can be used to effectively teach public health concepts and principles.























































































