
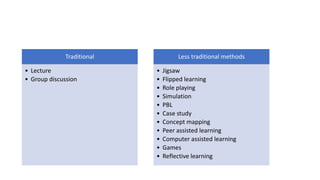
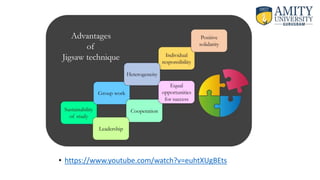


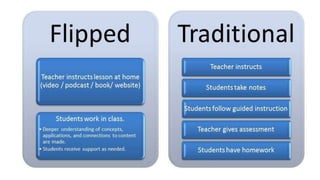






This document discusses various pedagogical approaches used in nursing education, including traditional lecture-based methods and more interactive techniques. It provides details on the jigsaw method, flipped classroom approach, simulation, and case-based learning. For each approach, it outlines how they work, examples of their implementation in nursing education, and research evaluating their effectiveness at improving student learning outcomes compared to traditional methods.

















![2nd yr bsc[n] cet ppt-methods of teaching -nsg education](https://cdn.slidesharecdn.com/ss_thumbnails/2ndyrbscncet-ppt-methodsofteaching-nsgeducation-200426055039-thumbnail.jpg?width=640&height=640&fit=bounds)





































































