Downloaded 212 times





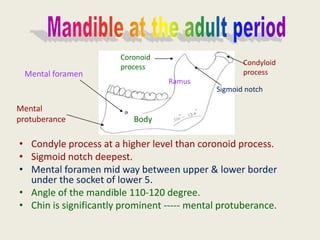




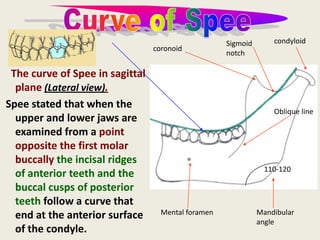
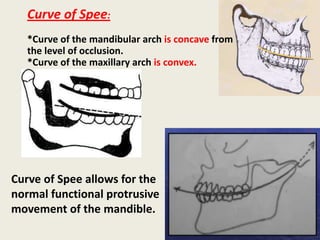



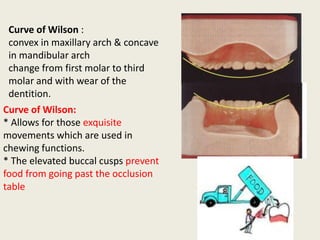





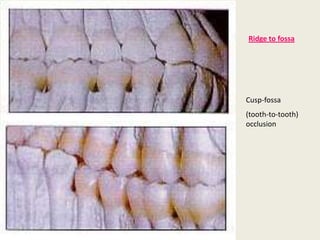




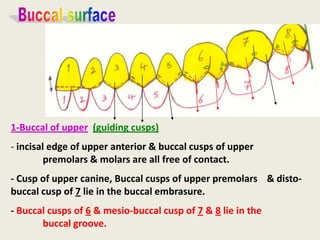












This document describes the anatomy and development of the mandible at different ages from birth through adulthood and old age. It discusses features such as the location of the condyle process, coronoid process, mental foramen, and mandibular canal. It also describes how the mandible changes with age, including the fusion of parts, changes in angles, and the levels of processes. Curves of the mandible and dental occlusion planes such as the curves of Spee, Wilson, and Monson are explained. Key aspects of normal occlusion like centric relation and the roles of teeth are summarized.











































![]Dental Occlusion part 1](https://cdn.slidesharecdn.com/ss_thumbnails/occlusionpart1-160420073612-thumbnail.jpg?width=640&height=640&fit=bounds)





















































