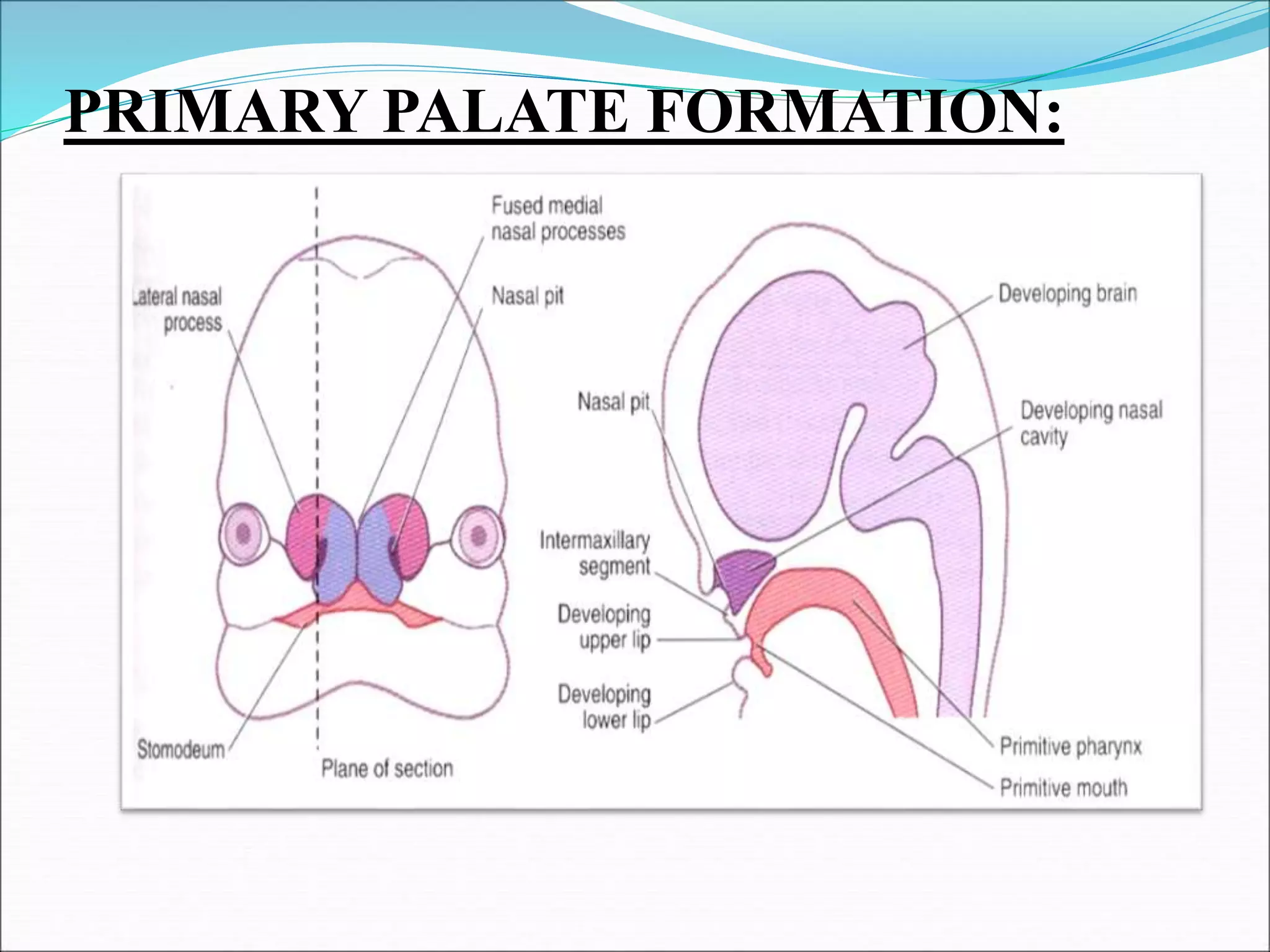
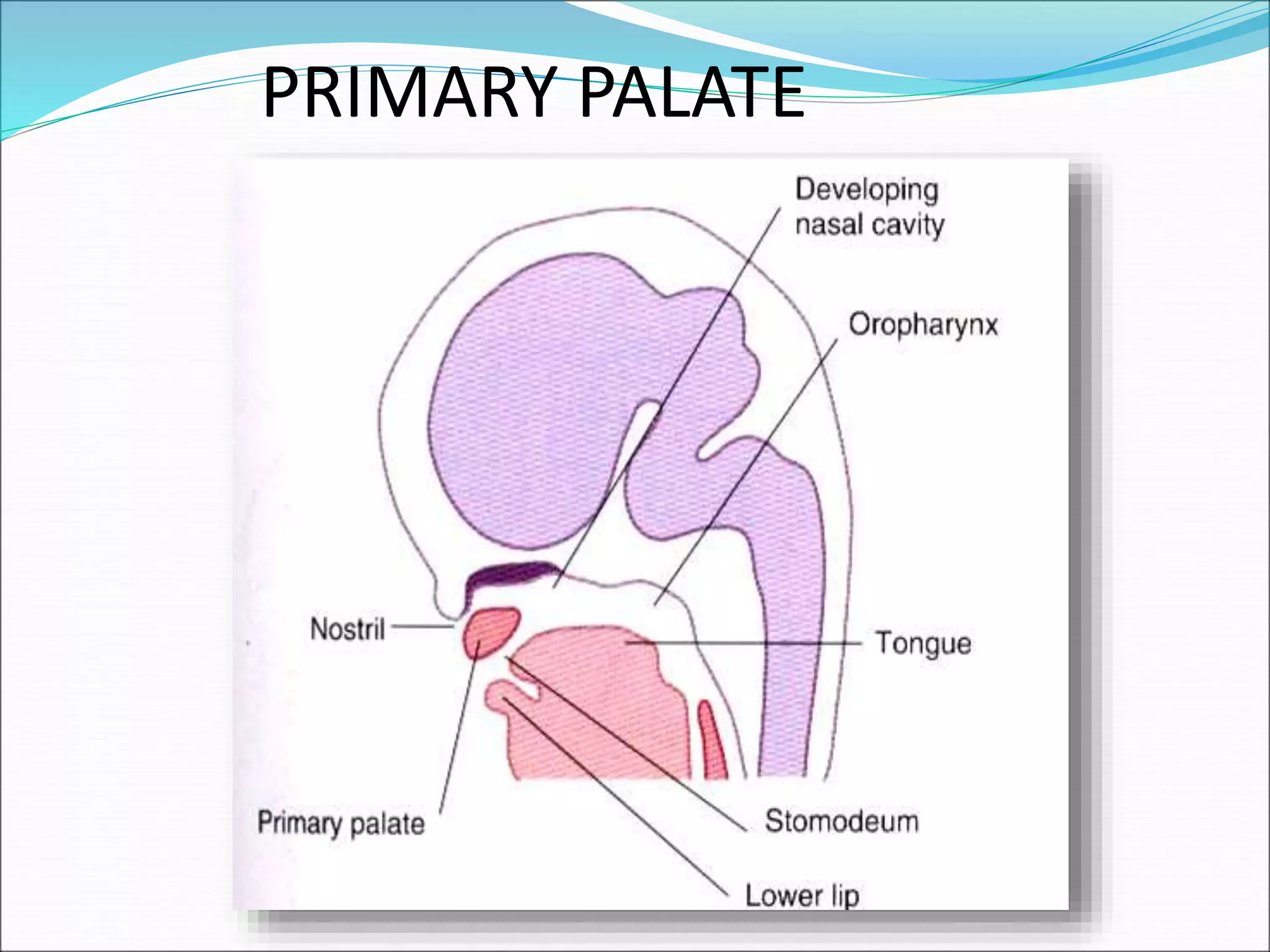
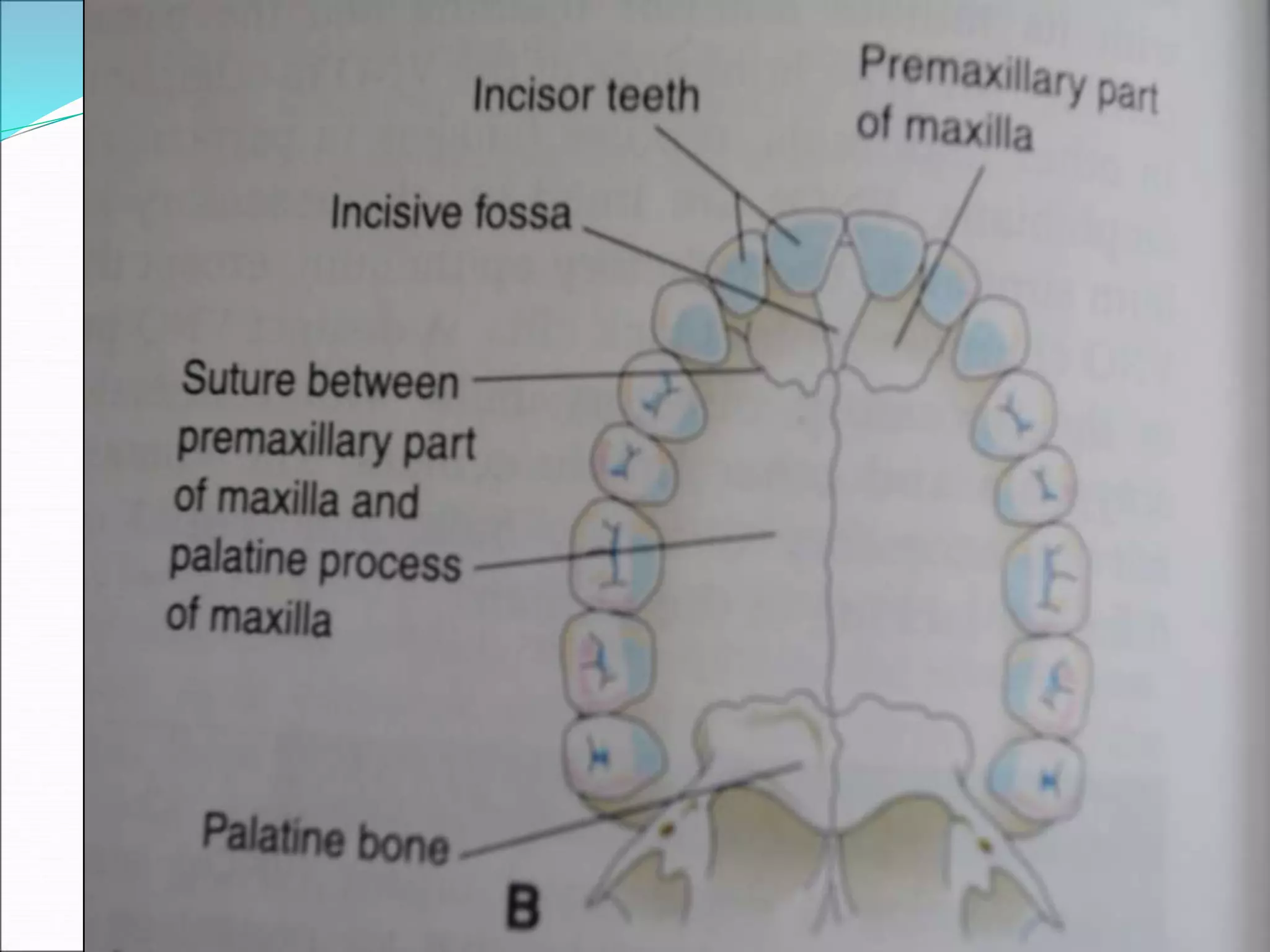
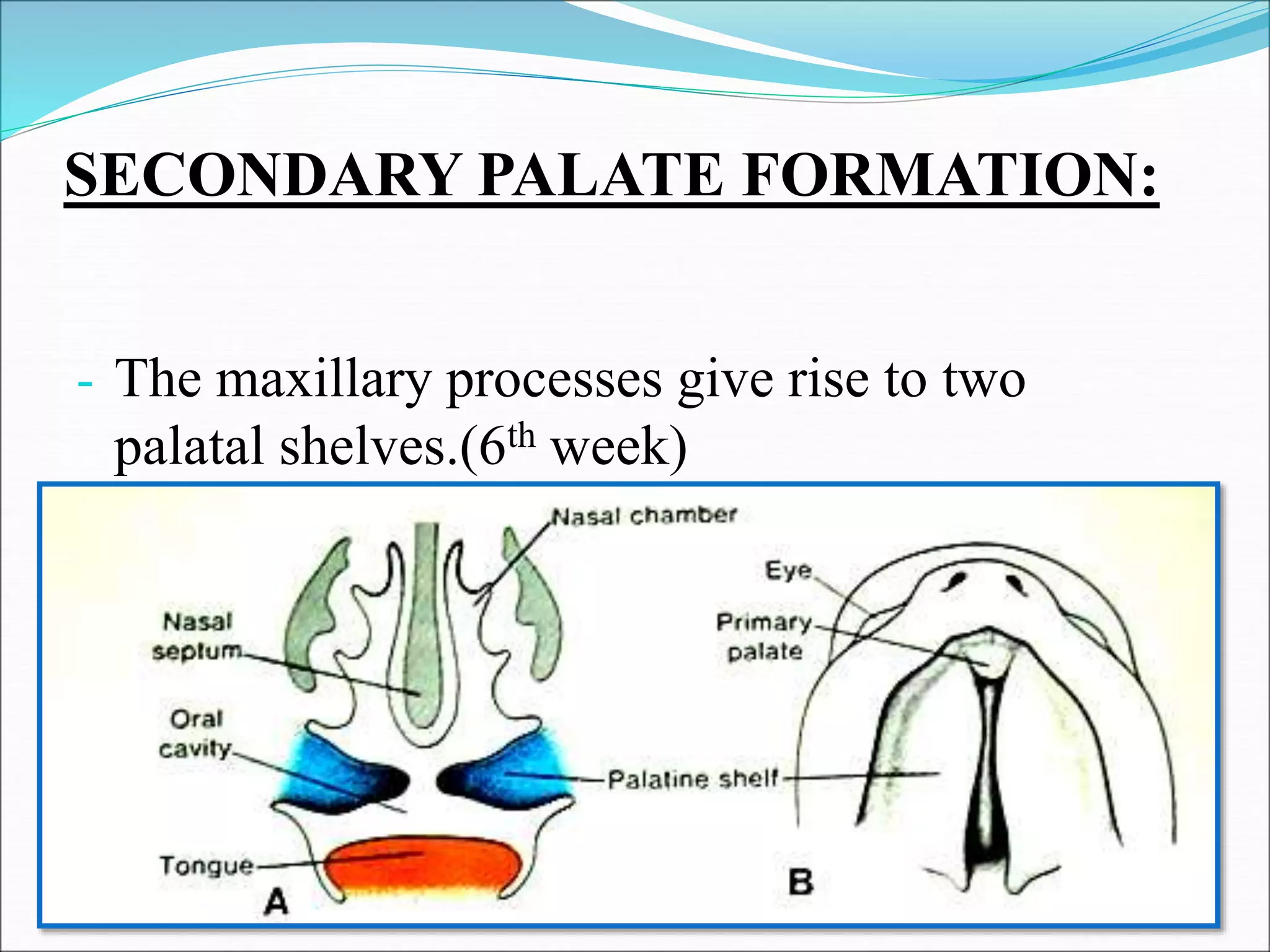
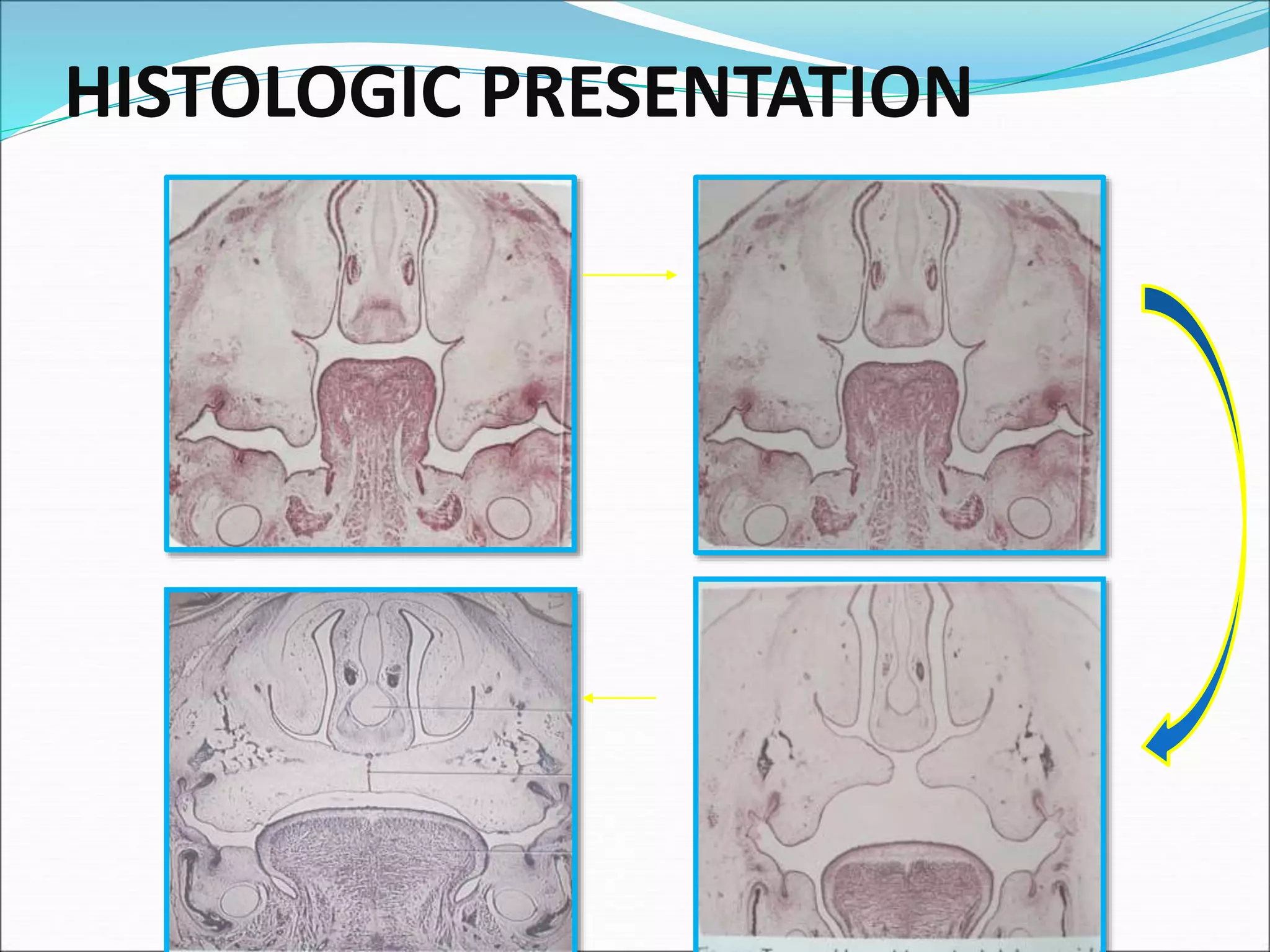
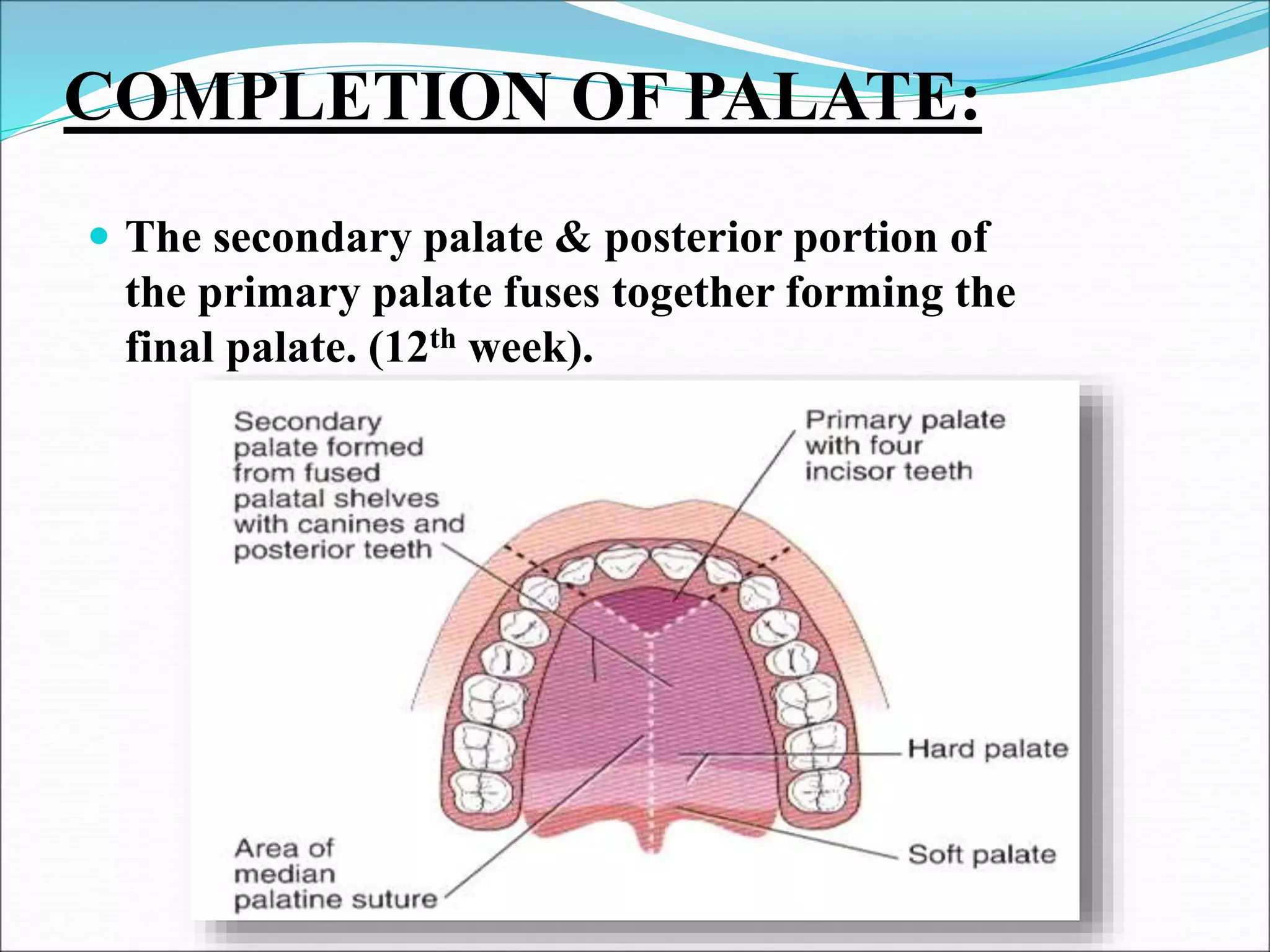
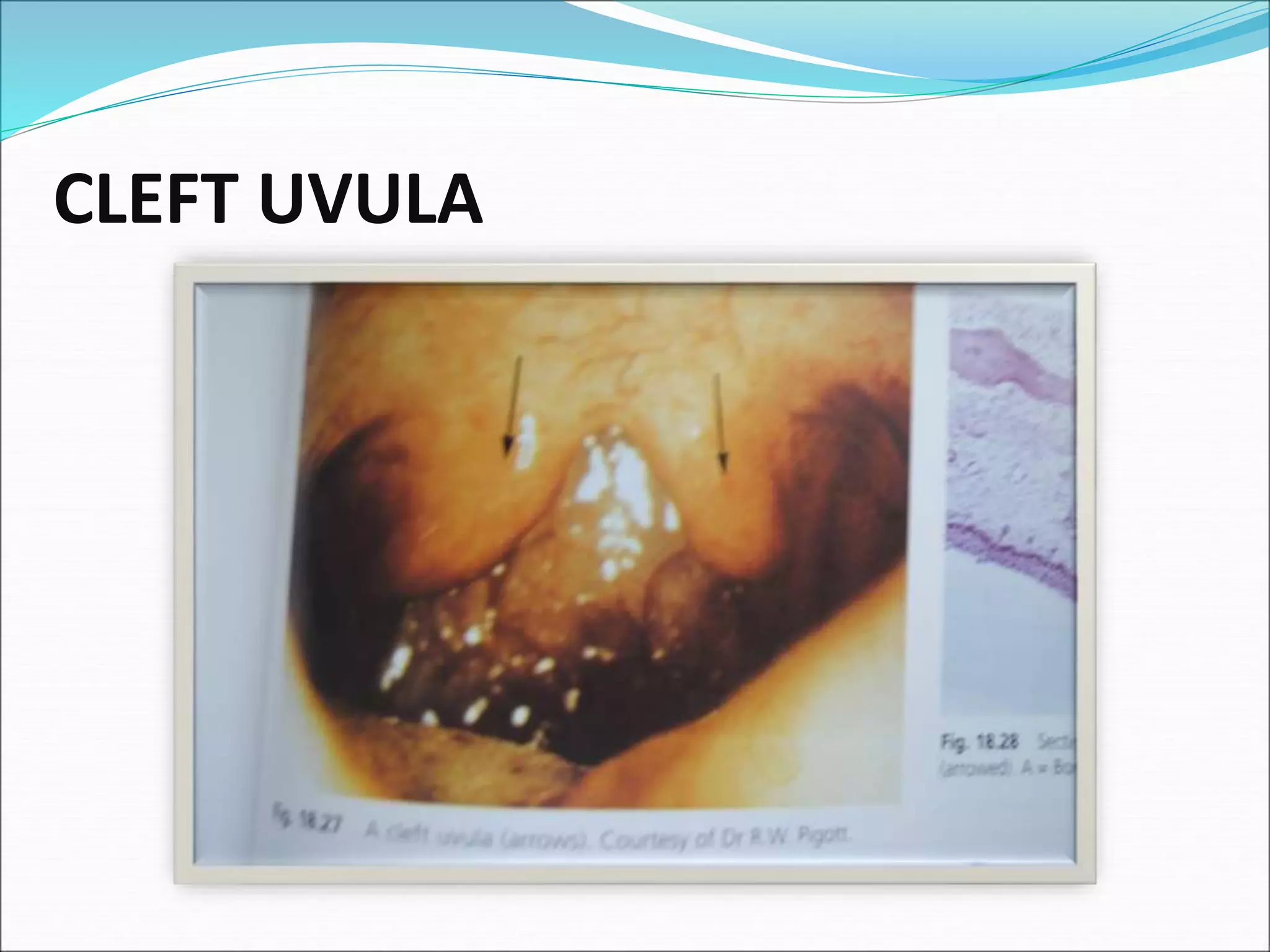
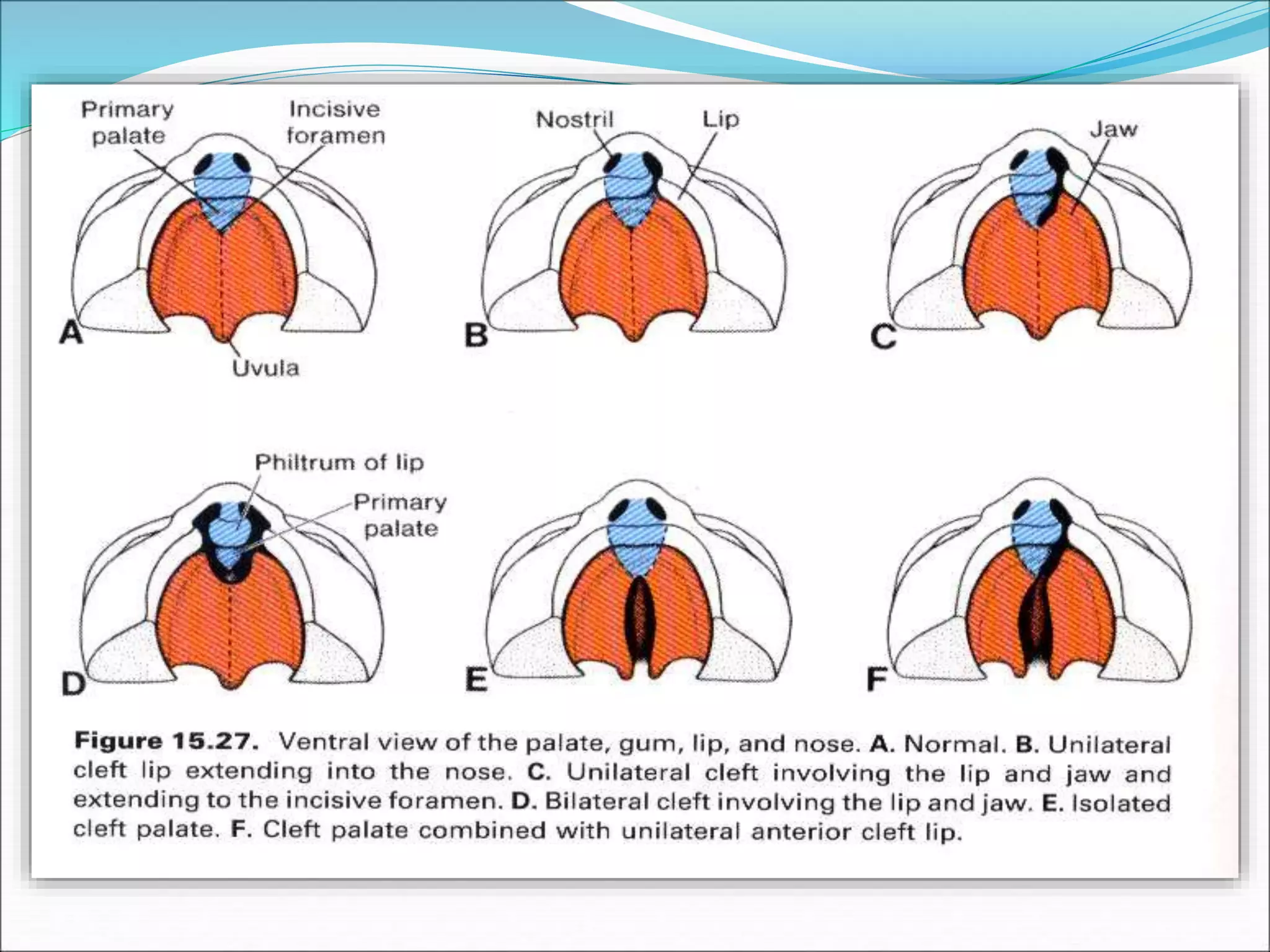
This document discusses the development of the palate. It begins by introducing the three components that make up the palate: the two lateral maxillary palatal shelves and the primary palate of the frontonasal prominence. It then describes the formation of the primary palate from the medial nasal processes in the 6th week of development. Next, it explains that the maxillary processes give rise to the two palatal shelves in the 6th week and that between the 8th-9th week the palatal shelves elevate and then fuse together in the 12th week to form the secondary palate. The document concludes by discussing various cleft lip and palate defects and syndromes associated with palate development.