

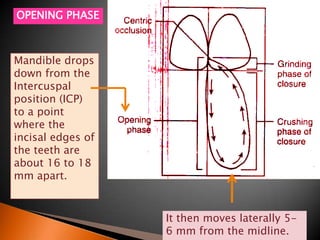
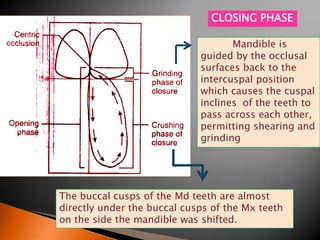
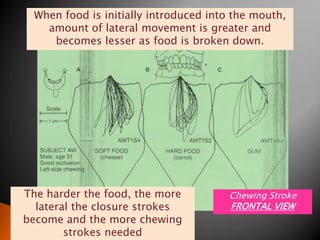
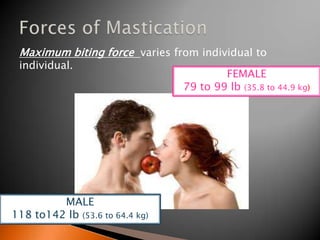
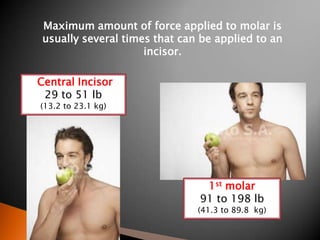

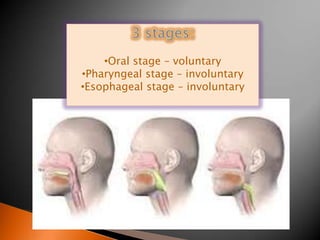
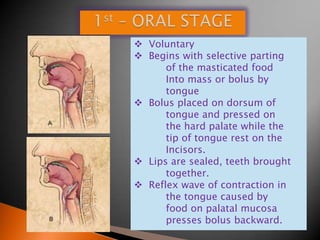
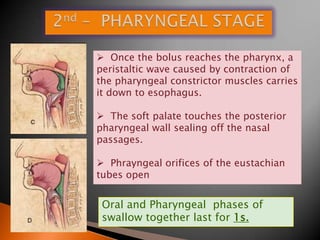
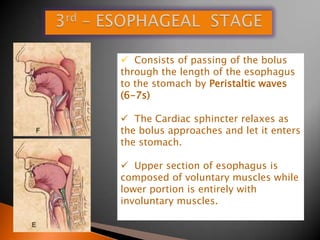

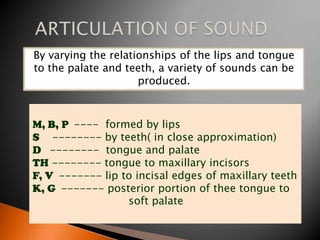
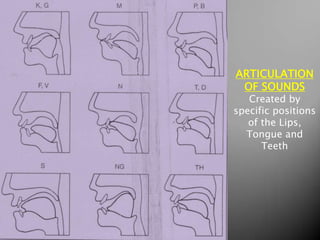

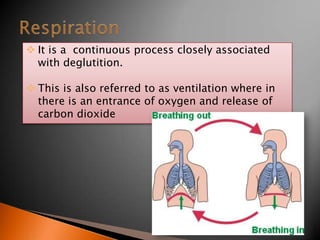
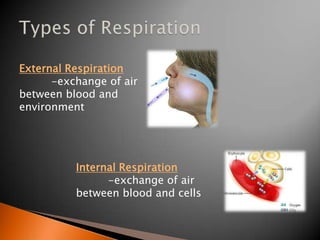
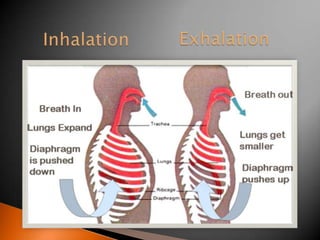


This document discusses several functions of the stomatognathic system including mastication, deglutition, speech, and respiration. It provides details on the physiology and mechanics of each function. For mastication, it describes the opening and closing phases, chewing strokes, and forces involved. Deglutition is summarized as a three stage process - oral, pharyngeal, and esophageal. Speech production involves respiration, phonation, resonance, and articulation using various positions of the lips, tongue, and teeth. Respiration is described as the exchange of air between the blood and environment.