Download as PDF, PPTX

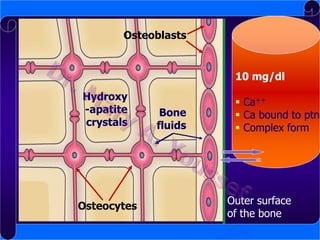
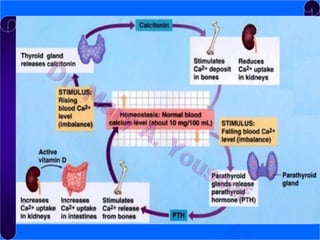
![Plasma calcium:
Its concentration is about 10mg/dl
1. Ionized 50%
2. Bound to protein 40%
3. Complex & diffusible form 10%
Solubility product:
[Ca2+] x [PO43-] = constant](https://image.slidesharecdn.com/endocrinesystem-physiology-131208133211-phpapp02/85/Endocrine-System-Physiology-57-320.jpg)




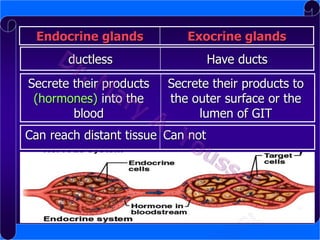
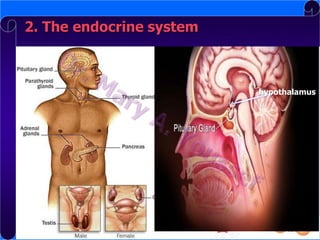
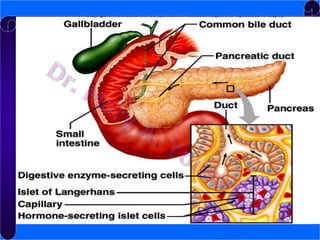
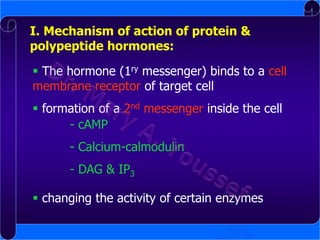
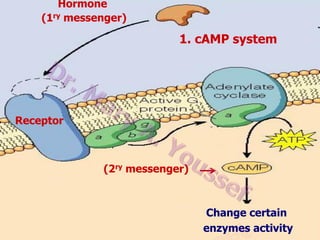
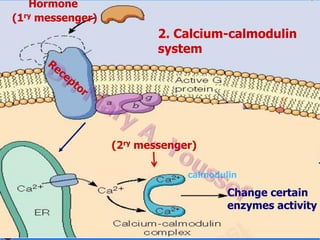
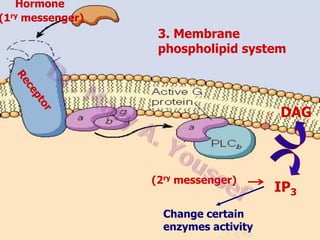
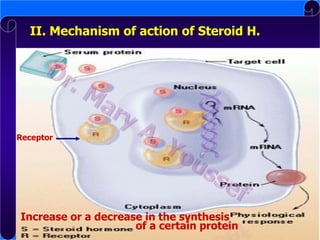
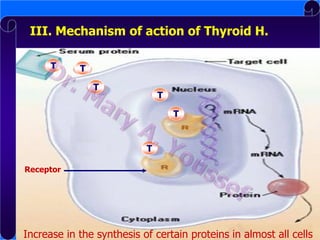
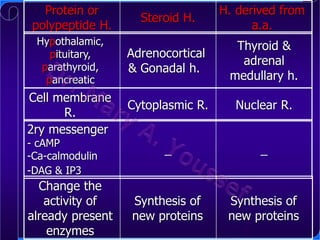
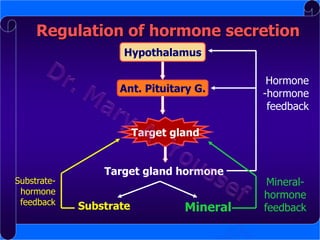
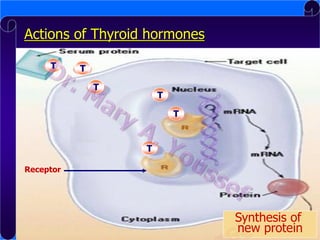
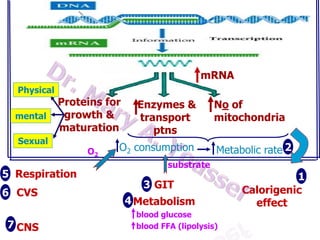
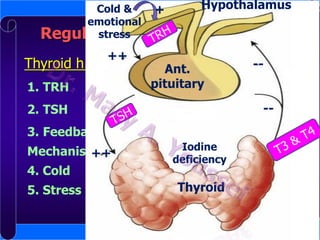
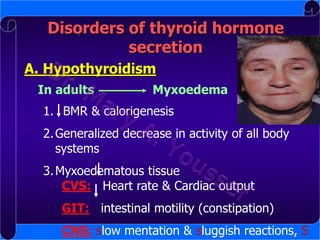
The document summarizes the key aspects of the endocrine system. It discusses the two main control systems - the nervous system and the endocrine system. It then focuses on the endocrine system, describing the endocrine glands and hormones. The mechanisms of hormone action and classifications of hormones are explained. Finally, it provides overviews of specific endocrine glands including the pituitary gland, thyroid gland, parathyroid glands, and adrenal glands.



































































































