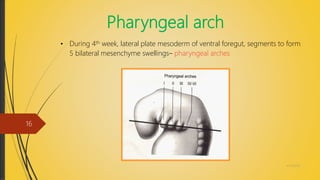
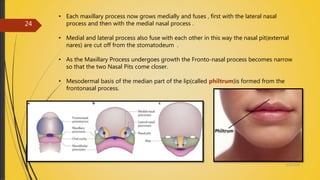
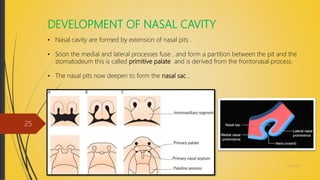
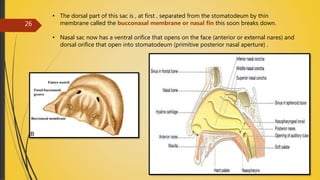
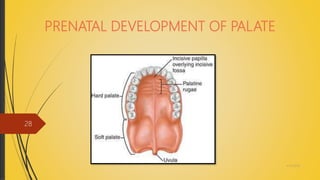
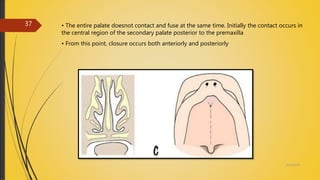
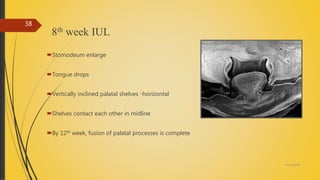
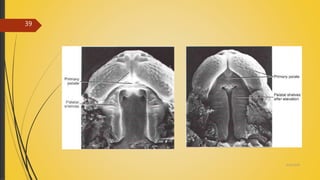
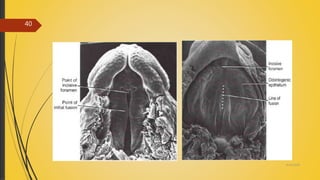
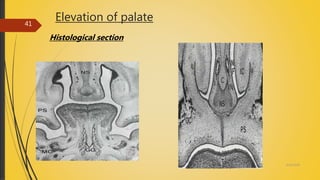
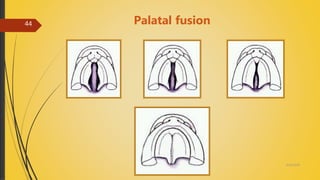
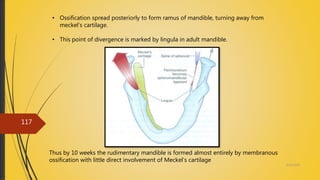
The document discusses the prenatal development of the maxilla and palate. It describes how during the 4th week of development, the maxillary processes arise from the first pharyngeal arches and grow medially to form the primary palate. Between the 6th-8th week, the secondary palate develops as the palatal shelves reorient horizontally and fuse in the midline. By the 12th week, fusion of the palatal processes is complete, separating the oral and nasal cavities.

















![Growth & development of maxilla & mandible.ppt [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/growthdevelopmentofmaxillamandible-180610064645-thumbnail.jpg?width=640&height=640&fit=bounds)










































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




