Downloaded 322 times
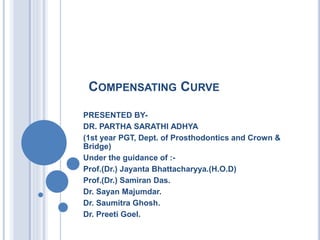
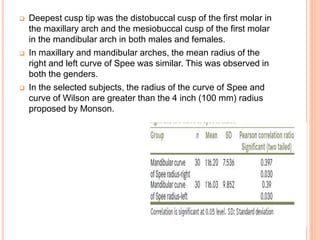
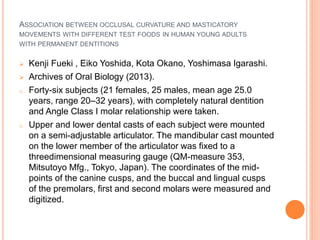
![CURVE OF MONSON [GEORGE S. MONSON, U.S.
DENTIST, 1869-1933]
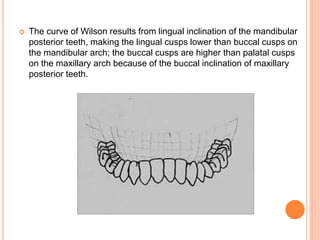
curve of occlusion in which each cusp and incisal edge
touches or conforms to a segment of the surface of a sphere 8
inches in diameter with its center in the region of the glabella.-
GPT-9
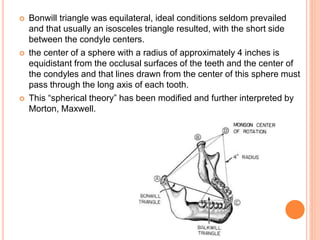
if jaw development was ideal, an equilateral triangle would be
formed by straight lines drawn connecting the centers of both
condyles and connecting these centers and a point at the
mesioincisal angle of the lower central incisors. – Bonwill.
the points on the lower jaw teeth which move in contact with
those in the skull lie on the surface of a sphere.- Von Spee.](https://image.slidesharecdn.com/curves-190103170916/85/Compensating-Curves-in-Prosthodontics-5-320.jpg)
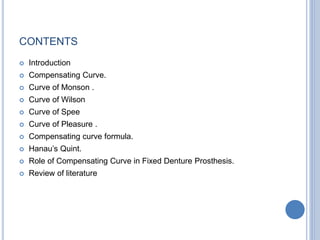
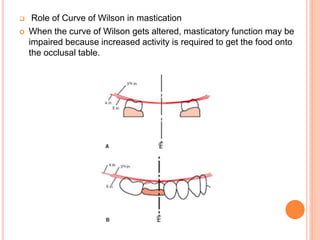
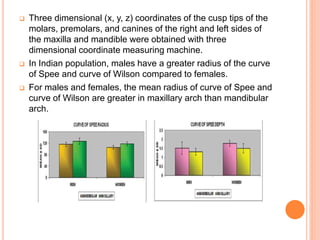
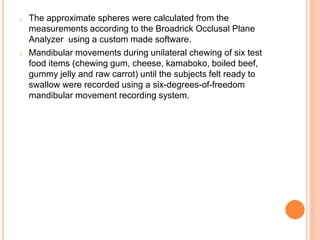
![CURVE OF WILSON [GEORGE H. WILSON, U.S.1855-
1922]
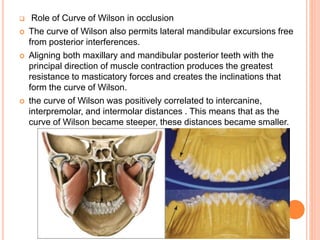
In the theory that occlusion should be spherical, the curvature
of the cusps as projected on the frontal plane expressed in
both arches; the curve in the mandibular arch being concave
and the one in the maxillary arch being convex.- GPT-9
the curve of Wilson also permits lateral mandibular excursions
free from posterior interferences](https://image.slidesharecdn.com/curves-190103170916/85/Compensating-Curves-in-Prosthodontics-8-320.jpg)
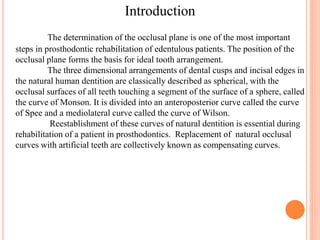
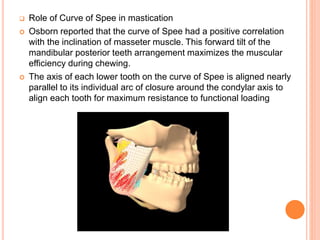
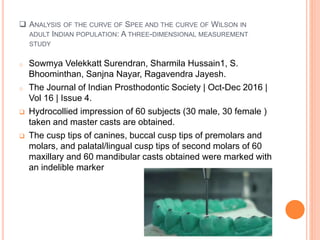
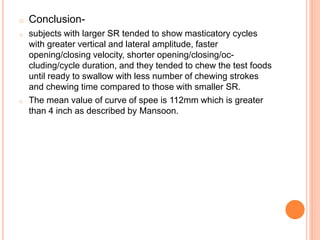
![CURVE OF SPEE [FERDINAND GRAF SPEE, PROSECTOR
OF ANATOMY, GERMANY, 1855-1937]:
The anatomical curve established by the occlusal alignment
of the teeth, as projected onto the median plane, beginning
with the cusp tip of the mandibular canine and following the
buccal cusp tips of the premolar and molar teeth, continuing
through the anterior border of the mandibular ramus and
ending at the anterior aspect of the mandibular condyle.-
GPT-8
The arc of a curved plane that is tangent to the incisal edges
and the buccal cusp tips of the mandibular dentition viewed in
the sagittal plane.](https://image.slidesharecdn.com/curves-190103170916/85/Compensating-Curves-in-Prosthodontics-12-320.jpg)
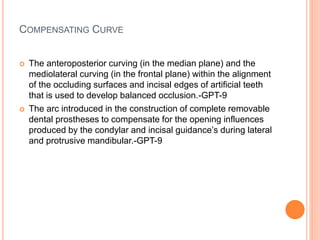
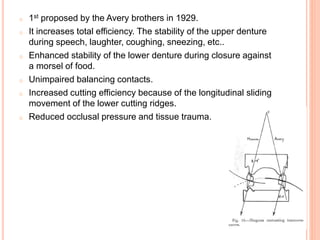
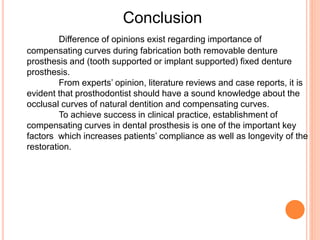
![CURVE OF PLEASURE [MAX A. PLEASURE,
U.S. DENTIST, 1903-1965]
A helicoid curve of occlusion that, when viewed in the frontal
plane, conforms to a mediolaterally convex curve in which the
lingual surfaces of the teeth are more coronal to the buccal
surfaces, except for the last molars, which reverse that
pattern.- GPT-9
in excessive wear of the teeth, the obliteration of the cusps
and formation of either flat or cuppedout occlusal surfaces,
associated with reversal of the occlusal plane of the premolar,
first and second molar teeth (the third molars being generally
unaffected), whereby the occlusal surfaces of the mandibular
teeth slope facially instead of lingually and those of the
maxillary teeth incline lingually.- GPT-9](https://image.slidesharecdn.com/curves-190103170916/85/Compensating-Curves-in-Prosthodontics-19-320.jpg)
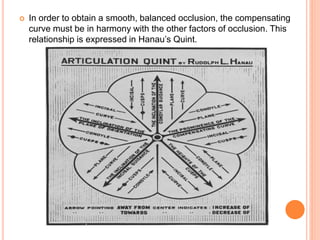
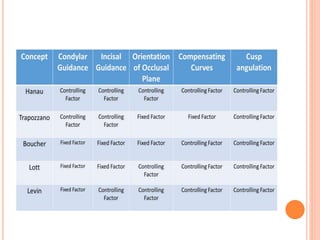
![HANAU’S QUINT
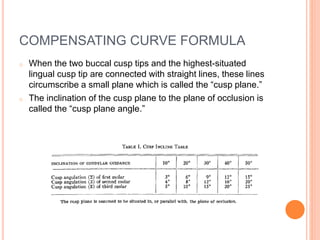
Rules for balanced denture articulation including incisal
guidance, condylar guidance, cusp length, the plane of
occlusion, and the compensating curve.-GPT-9
[K × I]/[OP × C × OK].
o K = the inclination of condylar guidance,
o I = the inclination of the incisal guidance,
o C = the height of the cusps,
o OP = the inclination of the plane of orientation,
o OK = the prominence of the compensating curve.](https://image.slidesharecdn.com/curves-190103170916/85/Compensating-Curves-in-Prosthodontics-27-320.jpg)
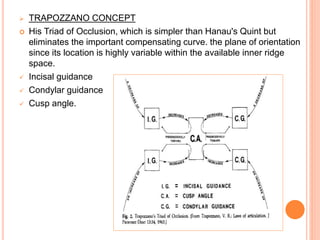


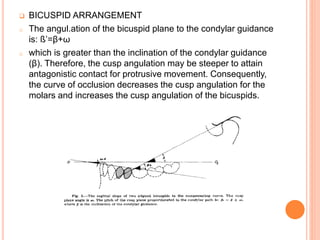
The document discusses compensating curves in prosthodontics, specifically how the curves of Monson, Wilson, and Spee relate to occlusal plane determination for fixed denture prostheses. It highlights their importance in achieving balanced occlusion for edentulous patients and includes findings from a study on the radii of these curves in Indian populations. Additionally, various philosophies regarding occlusion and denture construction, including Hanau’s quint and Pankey-Mann-Schuyler philosophy, are presented to illustrate the interplay between these curves and optimal denture design.














































































