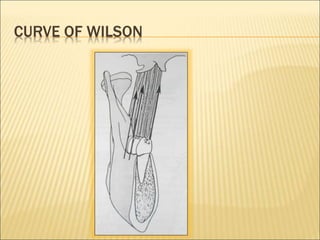
This document discusses concepts of occlusion including definitions of normal, ideal, physiologic, and pathologic occlusion. It describes static and dynamic occlusion as well as supporting and non-supporting cusps. Compensatory curves including the curves of Spee, Wilson, and Monson are explained. Posterior and anterior centric contacts, the plane of occlusion, centric relation, and centric occlusion are defined. The importance of understanding centric relation for orthodontic diagnosis and treatment planning is highlighted.