Call Girls Service in Bommanahalli - 7001305949 with real photos and phone nu...
CVS.pdf
1. USMLE Endpoint
C V S System
1 Dr/Ahmed Shebl
Embryology CVS
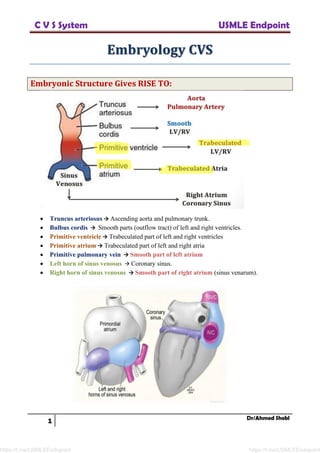
Embryonic Structure Gives RISE TO:
• Truncus arteriosus → Ascending aorta and pulmonary trunk.
• Bulbus cordis → Smooth parts (outflow tract) of left and right ventricles.
• Primitive ventricle → Trabeculated part of left and right ventricles
• Primitive atrium → Trabeculated part of left and right atria
• Primitive pulmonary vein → Smooth part of left atrium
• Left horn of sinus venosus → Coronary sinus.
• Right horn of sinus venosus → Smooth part of right atrium (sinus venarum).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
2. USMLE Endpoint
C V S System
2 Dr/Ahmed Shebl
Cardinal Veins:
• Form SVC/IVC (not from heart tube) → connect to right atrium.
• Superior vena cava → R common cardinal vein and R anterior cardinal vein.
• Inferior vena cava → Posterior subcardinal, and supracardinal veins.
• Venous system of the developing embryo:
➢ Vitelline veins → veins of the portal system.
➢ Umbilical → degenerate.
➢ Cardinal veins → veins of the systemic circulation e.g. SVC.
Heart morphogenesis:
• First functional organ in vertebrate embryos; beats spontaneously by week 4 of development.
Cardiac looping:
• Primary heart tube loops to establish left-right polarity; begins in week 4 of gestation.
• Establishes left-right orientation in chest.
• Requires cilia and dynein.
• Defect in left-right dynein (involved in L/R asymmetry) can lead to dextrocardia, as seen in
Kartagener syndrome (primary ciliary dyskinesia).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
3. USMLE Endpoint
C V S System
3 Dr/Ahmed Shebl
Septation of the chambers:
Atrial septation
1. Septum primum grows toward endocardial cushions, narrowing foramen primum.
2. Foramen secundum forms in septum primum (foramen primum disappears).
3. Septum secundum develops as foramen secundum maintains right-to-left shunt.
4. Septum secundum expands and covers most of the foramen secundum. The residual foramen
is the foramen ovale.
5. Remaining portion of septum primum forms valve of foramen ovale.
6. Septum secundum and septum primum fuse to form the atrial septum.
7. Foramen ovale usually closes soon after birth because of → LA pressure.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
4. USMLE Endpoint
C V S System
4 Dr/Ahmed Shebl
Patent foramen ovale:
• Caused by failure of septum primum and septum secundum to fuse after birth.
• Considered normal variant in adults (20-30%). Most are left untreated.
• Can lead to paradoxical emboli (venous thromboemboli that enter systemic arterial
circulation), similar to those resulting from an ASD.
• Remains closed as pressure in LA > RA → so, ↑RA pressure → RT to LT shunt →
hypoxemia.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
5. USMLE Endpoint
C V S System
5 Dr/Ahmed Shebl
Septation of the Ventricles:
1. Muscular ventricular septum forms. Opening is called interventricular foramen.
2. Aorticopulmonary septum rotates and fuses with muscular ventricular septum to form
membranous interventricular septum, closing interventricular foramen.
3. Growth of endocardial cushions separates atria from ventricles and contributes to both
atrial septation and membranous portion of the interventricular septum.
4. Ventricular Septum Pathology:
a. Membranous VSD (most common type)
b. Muscular VSD
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
6. USMLE Endpoint
C V S System
6 Dr/Ahmed Shebl
Endocardial Cushions
• Contribute to several cardiac structures:
▪ Atrial septum
▪ Ventricular septum
▪ AV valves (mitral/tricuspid)
▪ Semilunar valves (aortic/pulmonic)
• Endocardial cushion defects:
▪ Atrioventricular canal defects.
▪ Atrioventricular septal defects
▪ ASD, VSD, Valvular malformations
▪ Common in Down syndrome.
• UW: congenital MR + ostium primum ASD → endocardial cushion defect → mostly with
Down syndrome.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
7. USMLE Endpoint
C V S System
7 Dr/Ahmed Shebl
Aorticopulmonary septum: (Spiral Septum)
• Formed from neural crest cells → formation of truncal and bulbar ridges that spiral and
fuse to form aorticopulmonary septum.
• Separates aorta and pulmonary arteries.
• Fuses with interventricular septum.
Abnormal AP septum (conotruncal abnormalities):
1. Transposition of great vessels: Failure to spiral.
2. Tetralogy of Fallot:
a. Skewed septum development → Anterosuperior displacement of septum.
b. Abnormal neural crest cell migration.
3. Persistent truncus arteriosus: Partial/incomplete septum develop.
Valve development:
<
• Aortic/pulmonary: derived from endocardial cushions of outflow tract.
• Mitral/tricuspid: derived from fused endocardial cushions of the AV canal.
• Valvular anomalies may be stenotic, regurgitant, atretic (e.g., tricuspid atresia), or displaced
(e.g., Ebstein anomaly).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
8. USMLE Endpoint
C V S System
8 Dr/Ahmed Shebl
Shunts
• Left side pressures >> Right side pressures.
• Shunts → Left to right flow:
➢ VSD (LV → RV)
➢ ASD (LA → RA)
➢ PDA (Aorta → Left pulmonary artery)
• At birth:
➢ Left to right flow → volume overload of right heart.
➢ Blood flow to lungs unimpaired → no cyanosis.
• YEARS later (untreated):
➢ Pulmonary vessels become stiff/thick.
➢ Right ventricle hypertrophies.
➢ Right sided pressures rise.
➢ Shunt reverses (now R → L).
➢ Cyanosis occurs (Eisenmenger syndrome) → “Blue kids” not “blue babies”.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
9. USMLE Endpoint
C V S System
9 Dr/Ahmed Shebl
Congenital heart diseases
Right-to-left shunts (cyanotic heart diseases)
• Early cyanosis “blue babies.”
• Often diagnosed prenatally or become evident immediately after birth.
• Usually require urgent surgical treatment and/or maintenance of a PDA.
1- Persistent truncus arteriosus
• Truncus arteriosus fails to divide into pulmonary trunk and aorta due to lack of
aorticopulmonary septum formation (neural crest derivative).
• Most patients have accompanying VSD.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
10. USMLE Endpoint
C V S System
10 Dr/Ahmed Shebl
2- Transposition of great vessels
• Due to failure of the aorticopulmonary septum to spiral.
• Aorta leaves RV (anterior) and pulmonary trunk leaves LV (posterior) → separation of
systemic and pulmonary circulations.
• Not compatible with life unless a shunt is present to allow mixing of blood (eg, VSD, PDA,
or patent foramen ovale).
• Without surgical intervention, most infants die within the first few months of life.
• High incidence in infants of diabetic mothers.
3- Tricuspid atresia
• Absence of tricuspid valve and hypoplastic RV.
• Requires both ASD and VSD for viability.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
11. USMLE Endpoint
C V S System
11 Dr/Ahmed Shebl
4- Tetralogy of Fallot (T4)
• Caused by anterosuperior displacement of the infundibular septum.
• Most common cause of early childhood cyanosis.
• Pathophysiology:
1- Septum displaced (moves toward RV):
▪ Causes “overriding aorta” → 5-95% of aorta may lie over RV
▪ Causes VSD → Usually large (“non-restrictive”)
2- Infundibulum “Conus Arteriosus”:
▪ “Funnel” leading to pulmonic valve
▪ Develops from bulbus cordis → smooth, muscular structure at RV outflow to
PA.
3- “Infundibular stenosis”
▪ Subpulmonary stenosis → RV outflow tract obstruction.
▪ Abnormal pulmonary valve → Rarely main cause of obstruction
▪ Flow obstruction → RVH
• Components:
1- Pulmonary infundibular stenosis:
▪ Most important determinant for prognosis.
▪ Pulmonary stenosis forces right-to-left flow across VSD → RVH, “tet spells”
(often caused by crying, fever, and exercise due to exacerbation of RV
outflow obstruction).
2- Right ventricular hypertrophy (RVH)— boot-shaped heart on CXR
3- Overriding aorta
4- VSD
▪ Squatting: ↑ SVR, ↓ right-to-left shunt, improves cyanosis.
• Treatment: early surgical correction.
• Boot-shaped heart:
▪ Adult → RVH
▪ Infant → T4
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
12. USMLE Endpoint
C V S System
12 Dr/Ahmed Shebl
5- Total anomalous pulmonary venous return
• Pulmonary veins drain into right heart circulation (SVC, coronary sinus, etc).
• Associated with ASD and sometimes PDA to allow for right-to-left shunting to maintain CO.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
13. USMLE Endpoint
C V S System
13 Dr/Ahmed Shebl
6- Ebstein anomaly
• Characterized by displacement of tricuspid valve leaflets downward into RV, artificially
“atrializing” the ventricle.
• Can be caused by lithium exposure in utero.
• C/P:
▪ Tricuspid regurge → right sided HF.
▪ Dilated RA → ↑ risk of SVT.
▪ Accessory conduction pathways → WPW syndrome.
7- Complete AV canal defect:
• AV canal contributes to the formation of the AV valves (ie, mitral and tricuspid valves) and
the AV septum.
• Complete absence → single common AV valve, which is often associated with regurgitation.
• Strong association with down syndrome.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
14. USMLE Endpoint
C V S System
14 Dr/Ahmed Shebl
Right to left shunts (Acyanotic heart diseases)
• Acyanotic at presentation; cyanosis may occur years later.
1- Ventricular Septal Defect (VSD)
• Most common congenital anomaly.
• Communication LV/RV → harsh, holosystolic murmur → Tricuspid area (LLSB).
• O2 saturation increases in RV and pulmonary artery.
• Characterized in many ways: • Size • Location • Associated defects.
• Small VSD:
➢ Resists flow across defect (“restrictive”) → lots of turbulence → loud murmur.
• Large VSD:
➢ Large hole (“non-restrictive”) → significant shunting.
➢ May lead to LV overload and HF → often closed surgically.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
15. USMLE Endpoint
C V S System
15 Dr/Ahmed Shebl
2- Atrial septal defect (ASD)
• Communication between left/right atrium → adds volume to RA/RV.
• Type of murmurs associated:
➢ Delays closure of pulmonic valve → wide, fixed splitting of S2.
➢ Increased flow across PV/TV → systolic ejection murmur.
➢ Rarely a mid-diastolic murmur
• O2 saturation increases in RA, RV, and pulmonary artery.
• May lead to paradoxical emboli (systemic venous emboli use ASD to bypass lungs and
become systemic arterial emboli).
Secundum type ASD:
• Most common.
• Defects at site of foramen ovale/ostium secundum:
➢ Poor growth of secundum septum
➢ Or excessive absorption of primum septum
• Located mid-septum.
• Often isolated defect.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
16. USMLE Endpoint
C V S System
16 Dr/Ahmed Shebl
• Patent foramen ovale Vs. ASD:
▪ PFO → failure of fusion of septum primum and septum secundum.
▪ Secundum ASD → defect in primitive atrium.
Primum type ASD
• Failure of the septum primum to fuse completely with the endocardial cushions leaves a
persistent ostium primum.
• Located near AV valves (the lower part of the interatrial septum).
• Often occurs with other defects.
• These patients usually also have:
➢ Cleft in the anterior leaflet of the mitral valve as well as in the septal leaflet of the
tricuspid valve, causing regurgitation through the AV valves.
• Seen in endocardial cushion defects (Down syndrome).
3- Patent ductus arteriosis
• Ductus arteriosus shunts blood in utero: Left pulmonary artery → aorta.
• Closes close after birth:
➢ “Functional” closure 18 to 24 hours (smooth muscle)
➢ “Anatomic” occlusion over next few days/weeks
• Becomes ligamentum arteriosum.
• Patency maintained by prostaglandin E2 (major source in utero is placenta).
➢ Alprostadil:
▪ Prostaglandin E1 → maintains patency of ductus arteriosus.
▪ Key effect: delivers blood to lungs.
▪ Useful when poor RV → PA blood flow
• Tetralogy of Fallot
• Pulmonary atresia
➢ Indomethacin:
▪ NSAID that inhibits cyclooxygenase → decreases prostaglandin formation.
▪ Can be used to close PDA.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
17. USMLE Endpoint
C V S System
17 Dr/Ahmed Shebl
• PDA is associated with congenital rubella syndrome:
➢ Mother: Rash, fever, lymphadenopathy.
➢ Baby: Deafness, cataracts, cardiac disease (PDA common).
➢ Rare in developed countries (vaccination).
➢ Consider in infants whose mothers are immigrants.
• Uncorrected PDA can cause differential cyanosis:
➢ Occurs when shunt reverses R → L
➢ Blue toes, normal fingers
4- Eisenmenger’s Syndrome
• Uncorrected ASD/VSD/PDA → Right heart chronically overloaded → RV Hypertrophy →
Pulmonary hypertension.
• Shunt reverses right >> left (bypassing lung).
▪ Cyanosis, Clubbing, Polycythemia (very high Hct).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
18. USMLE Endpoint
C V S System
18 Dr/Ahmed Shebl
Coarctation of aorta
• Aortic narrowing near insertion of ductus arteriosus (“juxtaductal”).
• Subtypes based on location of ductus arteriosus.
Preductal or Infantile type:
• Symptoms varies according the patency of ductus arteriosus:
• Open ductus arteriosus: (at birth)
➢ Ductus arteriosus supplies lower extremities.
➢ Deoxygenated blood to lower extremity → lower extremity cyanosis may occur.
• Ductus closure:
➢ All flow through aorta with severe narrowing → abrupt increase afterload.
➢ Rise in LVEDP → Acute heart failure.
➢ LV can dilate → fail → shock.
➢ Poor development of collateral vessels.
• Key associations: Turner syndrome (45, XO).
Postductal or Adult type:
• Ductus arteriosus does not supply lower extremities
• Collaterals develop.
• May go undetected until adulthood.
• Lower extremities → low blood pressure → ↑ Renin release → Salt/water retention →
Vasoconstriction (AII) → Weak pulses (“brachio-femoral delay”)
• Upper extremities and head → high blood pressure → Secondary hypertension.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
19. USMLE Endpoint
C V S System
19 Dr/Ahmed Shebl
Associations of coarctation
1. Bicuspid aortic valve:
a. Found in up to 60% of coarctation cases.
b. The most common associated anomaly with turner.
c. Early systolic + high frequency click over the apex.
d. Can be present also with AR murmur.
e. Associated with premature calcification at the 6th
decade (normally aortic valve
calcification occurs at 8th
to 9th
decades) → aortic stenosis.
f. Most common cause of congenital aortic stenosis is calcification of bicuspid aortic
valve.
g. NB: Coarctation + murmur → AR d2 bicuspid aortic valve.
2. Intracranial aneurysms: Occur in about 10% of patients with coarctation.
3. Turner syndrome.
Signs and symptoms of coarctation of aorta
• Hypertension in upper extremities.
• Weak delayed pulse in lower extremities (brachial-femoral delay).
• Murmur over back between scapula.
• With age, intercostal arteries enlarge due to collateral circulation; arteries erode ribs →
notched ribs on CXR.
• 3‐sign: Bulge before and after coarctation on chest x-ray.
Complications of coarctation of aorta
• HF: pressure overload on the LV.
• ↑ Risk of cerebral hemorrhage (berry aneurysms).
• Aortic rupture/ dissection.
• Endocarditis/endarteritis:
➢ High-low pressure across narrowing → Endothelial injury.
➢ Low pressure distal to narrowing → Bacteria may attach more easily.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
20. USMLE Endpoint
C V S System
20 Dr/Ahmed Shebl
• UW: Differential clubbing and cyanosis:
▪ Without blood pressure or pulse discrepancy are pathognomonic for a large patent
ductus arteriosus complicated by Eisenmenger syndrome (reversal of shunt flow
from left-to-right to right-to-left).
▪ With BP or pulse discrepancy → Severe preductal coarctation of the aorta.
Congenital heart disease associations
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
21. USMLE Endpoint
C V S System
21 Dr/Ahmed Shebl
Fetal erythropoiesis
,
• Fetal erythropoiesis occurs in:
▪ Yolk sac (3–8 weeks)
▪ Liver (6 weeks–birth)
▪ Spleen (10–28 weeks)
▪ Bone marrow (18 weeks to adult)
▪ Young Liver Synthesizes Blood.
Hemoglobin development
• Embryonic globins: ζ and ε.
• Fetal hemoglobin (HbF) = α2γ2.
• Adult hemoglobin (HbA) = α2β2.
• NB: HbF has higher affinity for O2 due to less avid binding of 2, 3-BPG, allowing HbF to
extract O2 from maternal Hemoglobin HbA1 and HbA2) across the placenta.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
22. USMLE Endpoint
C V S System
22 Dr/Ahmed Shebl
Fetal circulation
➢ UW: the highest value of O2 saturation is recorded in IVC in fetal circulation. As it carries
oxygenated blood from umbilical veins.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
23. USMLE Endpoint
C V S System
23 Dr/Ahmed Shebl
Fetal-postnatal derivatives
Ligamentum teres:
• Remnant of umbilical vein.
• Lies within the free edge of the darker falciform ligament, which attaches the liver to both
the diaphragm and the anterior abdominal wall.
• Divides the anatomic left and right lobes of the liver and easily seen as a darker structure
on CT because it contains some fat.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
24. USMLE Endpoint
C V S System
24 Dr/Ahmed Shebl
ANATOMY OF CVS
Anterior-Posterior Structures
• Right ventricle → Anterior:
✓ Injured if penetrating trauma at the mid and lower-left sternal border.
✓ The parietal pleura would be injured as well, but the left lung itself would not be
punctured as there is no middle lobe on the left side, and the superior lobe of the left lung is
displaced laterally by the cardiac impression.
• Left atrium → Posterior.
✓ Enlargement can cause dysphagia (due to compression of the esophagus) or hoarseness (due
to compression of the left recurrent laryngeal nerve, a branch of the vagus nerve).
✓ The closest to the probe of transesophageal ECHO.
✓ If the probe is placed posterior → descending aorta will be faced.
✓ The left atrial appendage is particularly susceptible to thrombus formation.
• Left ventricle → the left lateral aspect of the heart.
✓ A stab wound angled slightly medially in the fourth intercostal space at the midclavicular
line could strike the left ventricle, but only after passing through the bulk of the left lung.
• Right atrium → right border of the heart.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
25. USMLE Endpoint
C V S System
25 Dr/Ahmed Shebl
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
26. USMLE Endpoint
C V S System
26 Dr/Ahmed Shebl
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
27. USMLE Endpoint
C V S System
27 Dr/Ahmed Shebl
Surface anatomy of the heart:
• 2×3=6 + apex
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
28. USMLE Endpoint
C V S System
28 Dr/Ahmed Shebl
Anatomy of the conduction system
Anatomy of the AV node
• Location:
▪ The AV node is located on the endocardial surface of the right atrium, near the
insertion of the septal leaflet of the tricuspid valve and the orifice of the coronary
sinus.
• Radiofrequency ablation:
▪ Performed in patients with arrhythmia who do not respond to pharmacologic therapy.
▪ Locations:
▪ To the AV node is occasionally.
▪ Another area frequently involved in atrial fibrillation pathogenesis is the opening of
the pulmonary veins in the left atrium; this area is often a target for radiofrequency
ablation, but it is not where the AV node is located.
Anatomy of the SA node
• Located in the upper anterior right atrium at the opening of the superior vena cava.
Biventricular peacemaker of the heart
• A device that requires 2 or 3 leads:
▪ If 3 leads are used, the first 2 are placed in the right atrium and right ventricle.
▪ The third lead is used to pace the left ventricle.
• Right atrial and ventricular leads:
▪ Easy to place as they only need to traverse the left subclavian vein and superior vena
cava to reach these cardiac chambers.
• Left ventricular lead:
▪ More difficult to position. The preferred transvenous approach involves passing the
left ventricular pacing lead from the right atrium into the coronary sinus, which
resides in the atrioventricutar groove on the posterior aspect of the heart it is then
advanced into one of the lateral venous tributaries in order to optimize left
ventricular pacing.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
29. USMLE Endpoint
C V S System
29 Dr/Ahmed Shebl
• UW: coronary sinus:
▪ Venous drainage of the heart.
▪ Opens in the RA and normally not seen by ECHO.
▪ So, coronary sinus dilatation → is d2 increase in the RT side pressure because of
pulmonary HTN.
Blunt aortic injury (traumatic aortic rupture)
• Mechanism:
✓ Sudden deceleration that results in extreme stretching and torsional forces affecting the heart
and aorta.
✓ Injury occurs most often at the aortic isthmus:
▪ Proximal descending aorta just distal to origin of left subclavian artery.
▪ which is tethered by the ligamentum arteriosum and is relatively fixed and immobile
compared to the adjacent descending aorta.
• Clinically:
✓ The majority (80%) of patients die from aortic rupture before reaching the hospital.
✓ Those who survive the initial injury have nonspecific findings such as chest pain, back pain,
or shortness of breath.
✓ A widened mediastinum may also be seen on chest x-ray.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
30. USMLE Endpoint
C V S System
30 Dr/Ahmed Shebl
Coronary artery anatomy
• LAD supplies:
✓ Anterior surface of the LV.
✓ Anterior 2/3 of interventricular septum.
✓ Anterolateral papillary muscle.
✓ Most commonly occluded.
• PDA supplies:
✓ AV node (dependent on dominance).
▪ AV nodal artery arises from PDA (if rt dominant) or from LCX (if left dominant).
✓ Posterior 1/3 of interventricular septum.
✓ Posterior 2/3 walls of ventricles, and posteromedial papillary muscle.
✓ Right (acute) marginal artery supplies RV.
✓ Diaphragmatic surface of the heart (composed mainly from RV).
• RCA supplies:
✓ SA node (blood supply independent of dominance).
▪ Infarct may cause nodal dysfunction (bradycardia or heart block).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
31. USMLE Endpoint
C V S System
31 Dr/Ahmed Shebl
• Dominance:
✓ Right-dominant circulation (85%) = PDA arises from RCA.
✓ Left-dominant circulation (8%) =PDA arises from LCX.
✓ Codominant circulation (7%) = PDA arises from both LCX and RCA.
• Coronary blood flow peaks in early diastole.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
32. USMLE Endpoint
C V S System
32 Dr/Ahmed Shebl
• Papillary muscles of the mitral valve:
✓ Post. papillary muscle supplied only by PDA.
✓ Ant. papillary muscle has dual blood supply by LAD & LCX → less likely to rupture after
MI.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
33. USMLE Endpoint
C V S System
33 Dr/Ahmed Shebl
• UW: The optimal site for obtaining vascular access in the lower extremity during cardiac
catheterization is the common femoral artery below the inguinal ligament. Cannulation above the
inguinal ligament can significantly increase the risk of retroperitoneal hemorrhage.
Pericardium:
• Consists of 3 layers (from outer to inner):
▪ Fibrous pericardium.
▪ Parietal layer of serous pericardium.
▪ Visceral layer of serous pericardium.
• Pericardial cavity lies between parietal and visceral layers.
▪ Accumulation of fluid in the pericardial cavity compresses the heart, resulting in cardiac
tamponade.
• Pericardium innervated by phrenic nerve.
▪ Pericarditis can cause referred pain to the neck, arms, or one or both shoulders (often left).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
34. USMLE Endpoint
C V S System
34 Dr/Ahmed Shebl
CVS PHYSIOLOGY
Important Terms
• Stroke Volume (SV) = EDV -ESV
• Ejection Fraction (EF) = SV /EDV
• Cardiac Output (CO) = SV * HR
• Venous Return (VR)
▪ Blood returned to left ventricle
▪ Should be equal to the cardiac output
• Total peripheral resistance
▪ Resistance to blood flow from peripheral structures
▪ Vasoconstriction → ↑ TPR
▪ Vasodilation → ↓ TPR
• Systolic blood Pressure (SBP)
▪ Largely determined by stroke volume
• Diastolic blood Pressure (DBP)
▪ Largely determined by TPR
• Pulse pressure = SBP – DBP
▪ Proportional to SV
• Mean arterial pressure (MAP) = 2/3 DBP + 1/3 SBP
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
35. USMLE Endpoint
C V S System
35 Dr/Ahmed Shebl
Cardiac output
• More cardiac output = more work → more O2 demand
▪ CO = HR x SV
• Determinants of cardiac output:
▪ Stroke volume
▪ Contractility
▪ Preload
▪ Afterload
▪ Heart rate
• CO = rate of O2 consumption / arteriovenous O2 content difference.
▪ The rate of oxygen consumption can be determined with an oxygen meter by measuring the
rate of disappearance of oxygen in exhaled air.
Stroke volume
• Stroke Volume affected by Contractility, Afterload, and Preload.
• ↑ SV with:
1. Contractility (eg, anxiety, exercise).
2. ↓ Preload (eg, early pregnancy).
3. ↓ Afterload.
• A failing heart has ↓ SV (systolic and/or diastolic dysfunction).
Contractility
• How hard the heart muscle squeezes.
• Ejection fraction = index of contractility.
• Major regulator: sympathetic nervous system → also increases heart rate.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
36. USMLE Endpoint
C V S System
36 Dr/Ahmed Shebl
To INCREASE contractility (and SV) To DECREASE contractility (and SV)
1. Catecholamine stimulation via β-1
receptor:
a. Ca2+channels phosphorylated → Ca2+
entry → Ca2+_induced Ca2+ release
and ↑ Ca2+storage in sarcoplasmic
reticulum.
b. Phospholamban phosphorylation →
active Ca2+ATPase → ↑ Ca2+ storage
in sarcoplasmic reticulum.
2. ↑ Intracellular Ca2+
3. ↓ Extracellular Na+ (↓ activity of
Na+/Ca2+ exchanger).
4. Digitalis (blocks Na+/K+ pump → ↑
intracellular Na+ → ↓ Na+/Ca2+
exchanger activity → ↑ intracellular Ca2+)
1. β-1 blockade (↓ cAMP).
2. HF with systolic dysfunction.
3. Acidosis.
4. Hypoxia/hypercapnia.
5. Non-dihydropyridine Ca2+channel blockers.
Lusitropy:
• Myocardial relaxation.
• Mediated by SERCA.
1) SERCA is regulated by a protein called phospholamban (PLB).
▪ Phospholamban is an inhibitor to SERCA.
2) Sympathetic stimulation → phosphorylates PLB → ↓ PLB → ↑ SERCA → faster
relaxation → faster contraction.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
37. USMLE Endpoint
C V S System
37 Dr/Ahmed Shebl
Preload
• Amount of blood loaded into left ventricle.
• Also, how much stretch is on fibers prior to contraction.
▪ Some books say “length” instead of “stretch”.
▪ More preload = more cardiac output.
▪ More preload = more work the heart must do → more O2 is required.
To INCREASE Preload To DECREASE Preload
1. Add volume (blood, IVF)
2. Slow heart rate → more filling →more
volume
3. Constrict veins:
a. Veins force blood into heart
b. Veins hold LARGE blood volume
c. Response to blood loss → venous
constriction
d. Sympathetic stimulation → α1
receptors in veins
1. Remove volume (bleeding, dehydration)
2. Raise heart rate (opposite mechanism
above)
3. Pool blood in veins:
a. Mechanism of action of nitrates
b. Relieve angina
c. Lower preload → less work for heart
• Important Terms:
▪ LVEDV: Volume of blood in the left ventricle when filled.
▪ LVEDP: Pressure in the left ventricle when filled.
Afterload
• Forces resisting flow out of left ventricle.
• Heart must squeeze to increase pressure.
• Needs to open aortic valve → push blood into aorta.
• This is harder to do if:
▪ Blood pressure is high
▪ Aortic valve is stiff
▪ Something in the way: HCM, sub-aortic membrane
To INCREASE Afterload To DECREASE Afterload
1. Raise mean blood pressure.
2. Obstruct outflow of left ventricle: Aortic
stenosis, HCM.
1. Lower the mean blood pressure.
2. Treat aortic valve disease, HCM
a. More afterload = more work
b. More oxygen required
• LV compensates for increased afterload by thickening (hypertrophy) in order to decrease
wall tension.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
38. USMLE Endpoint
C V S System
38 Dr/Ahmed Shebl
Heart Rate
• Increases cardiac output under physiologic conditions.
• Mainly regulated by sympathetic nervous system.
• Also increased by sympathomimetic drugs.
• Decreased by beta blockers and calcium blockers.
• At pathologic heart rates ↑ HR = ↓ CO.
Cardiac output equations
❖ Venous vasodilators (eg, nitrogycerin) → ↓ preload.
❖ Arterial vasodilators (eg, hydralazine) → ↓ afterload.
❖ ACE inhibitors and ARBs ↓ both preload and afterload.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
39. USMLE Endpoint
C V S System
39 Dr/Ahmed Shebl
Work of the heart
• Myocardial oxygen demand is increased by:
1. ↑ Contractility.
2. ↑ Afterload (proportional to arterial pressure).
3. ↑ Heart Rate.
4. Diameter of ventricle (↑ wall tension).
• UW: perfusion of the heart is mainly during diastole. The systolic reduction of the coronary
flow is greatest in the subendocardial myocardium of the LV.
Cardiovascular Response to Exercise
• Process begins with muscle contraction → ATP consumed → oxygen consumed (need more
ATP) → Result: Local hypoxia in muscle tissue → Vasodilation occurs.
▪ Multiple VD mediators released into plasma:
▪ Adenosine generated from ATP consumption
▪ Lactate
▪ Carbon dioxide, potassium
▪ Vasodilatation → ↓ total peripheral resistance (TPR) → ↓ DBP.
• Sympathetic nervous system activated:
▪ Increase HR → ↑ CO (to meet the metabolic needs of the body).
▪ Results in ↑ systolic blood pressure (SBP).
▪ Venous constriction → ↑ preload → more ↑ CO.
▪ Vasoconstriction in some areas (gut, skin) → redistributes blood to important areas
(i.e. heart/muscles).
• NET result → “↑ SBP, ↓ DBP”
▪ Pulse pressure → increases.
▪ MAP → remains slightly constant (only increase 20-40).
• Fast HR → shortens diastole → LESS coronary filling time:
▪ Only way to get more oxygen is coronary vasodilation → increased blood flow.
▪ The heart cannot extract more O2 unlike other tissues.
▪ Cardiac tissue extracts maximum oxygen from RBCs.
▪ Cannot extract more to meet increased demand.
• KQB: Exercise has 2 types:
▪ Dynamic → increase blood flow d2 metabolic VD of arterioles.
▪ Static (weightlifting) → skeletal ms → compress BV → increase vascular resistance
→ decrease blood flow.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
40. USMLE Endpoint
C V S System
40 Dr/Ahmed Shebl
Lusitropy
• Lusitropy = myocardial relaxation “Opposite of contractility”
• Contributes to increased preload → ↑ cardiac output.
• Increased with exercise.
• Mediated by SERCA.
▪ SERCA takes up calcium → relaxation.
▪ SERCA is regulated by a protein called phospholamban (PLB).
▪ Phospholamban is an inhibitor to SERCA.
▪ Sympathetic stimulation “beta receptors” → phosphorylates PLB → ↓ PLB → ↑
SERCA → faster relaxation → faster contraction.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
41. USMLE Endpoint
C V S System
41 Dr/Ahmed Shebl
Flow Equations
• Flow “CO” = ΔP / TPR
• Flow (Q) = Velocity (V) * Area (A):
Resistance and Compliance
Total Peripheral Resistance
• Resistance to flow → more work for heart.
• What resists forward flow out of heart?
1. Types of vessels (i.e. pipes/tubes).
2. Thickness of blood (viscosity).
• Types of Vessels:
1. Arterioles = “resistance vessels” → major determinant of total peripheral resistance.
▪ Vasoconstriction = ↑ TPR, Vasodilation = ↓ TPR.
2. Veins provide most of blood storage capacity.
• Viscosity: depends mostly on hematocrit:
1. Low viscosity: Anemia.
2. High viscosity: Polycythemia, Multiple myeloma “hyperproteinemia”, Spherocytosis.
• Radius
o Changes in radius → large change in resistance.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
42. USMLE Endpoint
C V S System
42 Dr/Ahmed Shebl
Series and Parallel Circuits
• Human organs arranged in parallel.
• Resistances add up differently in series than in parallel.
• Organ removal “eg, nephrectomy” → ↑ TPR → ↓ CO.
• UW: removal of kidney or any other organ:
-↑ TPR (as organs are arranged in parallel)
-↓ CO
-normal arterial blood pressure (MAP= CO*TPR)
-↓ total renal blood flow (there is only one kidney)
Application of flow equation
• Flow “CO” = ΔP / Resistance.
• Blood flow to the body = CO
▪ ΔP = Arterial pressure – right atrial pressure
▪ R = Total peripheral resistance (TPR) = Systemic vascular resistance (SVR)
• Blood flow to the lungs = CO
▪ ΔP = Pulmonary artery pressure – left atrial pressure
▪ R = Pulmonary vascular resistance (PVR)
• Blood flow in systemic circulation is the same in pulmonary circulation.
▪ The pulmonary circulation is low resistant, high capacitance circulation.
Velocity and Area
• Flow (Q) = CO = Velocity (V) * Area (A).
• Cardiac output moves through system (same flow).
▪ Different vessels → different area, velocity
▪ Area ↑↑, velocity ↓↓
• Capillaries have highest total cross-sectional area and lowest flow velocity.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
43. USMLE Endpoint
C V S System
43 Dr/Ahmed Shebl
Flow Properties of Blood Vessels
Law of Laplace
• Wall tension or wall stress.
• Applies to vessels and cardiac chambers.
• ↑ Tension → ↑ O2 demand → ischemia/angina.
• Afterload: Increases pressure in left ventricle
▪ Hypertension, aortic stenosis → increase wall tension → “Pressure overload”.
• Preload: Increases radius of left ventricle
▪ Chronic valvular disease (aortic/mitral regurgitation) → increase wall tension →
“Volume overload”
Pressure overload Volume overload
▪ Due to increased afterload.
▪ Hypertension, aortic stenosis.
▪ Concentric hypertrophy to the ventricles:
o Sarcomeres added in parallel.
o Left ventricular mass increased
o Wall thickness increased
o Decreased compliance (stiff ventricle)
o Often seen in diastolic heart failure
▪ Due to increased preload.
▪ Chronic valvular disease.
▪ Eccentric hypertrophy to the ventricles:
o Sarcomeres added in series → Longer
myocytes.
o Left ventricular mass increased.
o Wall thickness NOT increased.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
44. USMLE Endpoint
C V S System
44 Dr/Ahmed Shebl
❖ KQB: old patient with wide pulse pressure HTN, why? → Aortic stiffness, as atherosclerosis
→ ↓ compliance → ↑ pulse pressure.
❖ Aortic regurge → volume overload → synthesis of new sarcomeres in series → eccentric
hypertrophy.
❖ Aortic stenosis → pressure overload → synthesis of new sarcomeres in parallel →
concentric hypertrophy.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
45. USMLE Endpoint
C V S System
45 Dr/Ahmed Shebl
Regulation of blood pressure
• Blood pressure is required for perfusion of tissues.
• Varies with sodium/water intake.
• Regulated by nervous system.
Baroreceptors
• Blood pressure sensors via stretch.
• Give signal central nervous system (brain).
• Response of the brain is via autonomic nervous system: Modify:
▪ Heart rate/contractility.
▪ Arterial tone (vasoconstriction).
▪ Venous tone (more tone = more preload to ventricle.)
▪ Renal renin release.
Aortic arch receptors Carotid sinus receptors
• Senses elevated blood pressure.
• Poor sensing of low blood pressure.
• Senses low and high blood pressure.
• Most important baroreceptor.
• Modifies signals over wider range of blood
pressure.
❖ Response to hypotension:
▪ ↓ Arterial pressure → ↓ stretch afferent baroreceptor firing → ↑ efferent sympathetic firing
and ↓ efferent parasympathetic stimulation → vasoconstriction, ↑ HR, ↑ contractility, ↑ BP.
▪ Important in the response to severe hemorrhage.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
46. USMLE Endpoint
C V S System
46 Dr/Ahmed Shebl
❖ Response to hypertension:
▪ Carotid massage → ↑ pressure on carotid sinus → ↑ stretch → ↑ efferent parasympathetic
firing → ↑ AV node refractory period → ↓ HR.
▪ Component of Cushing reflex:
✓ Triad of hypertension, bradycardia, and respiratory depression.
Chemoreceptors:
• Peripheral:
▪ Carotid and aortic bodies.
▪ Stimulated by ↓ Po2 (< 60 mm Hg), ↑ Pco2, and ↓ pH of blood.
• Central:
▪ Stimulated by changes in pH and Pco2 of brain interstitial fluid, which in turn are
influenced by arterial CO2.
▪ Do not directly respond to Po2.
Coronary Blood Flow
• The coronary artery fills during diastole.
• In tachycardia, less time in diastole → less flow.
• Epicardium → site of coronary arteries.
• Subendocardium receives smallest amount blood flow.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
47. USMLE Endpoint
C V S System
47 Dr/Ahmed Shebl
Cardiac circulation
• Three specific features distinguish cardiac circulation from blood flow to skeletal muscle and
viscera:
1. The heart is perfused only during diastole:
▪ Myocardial contraction during systole leads to compression of the coronary vessels and
disruption of blood flow.
▪ Wall tension is highest near the endocardium, making the subendocardial region the
most prone to ischemia.
2. Myocardial oxygen extraction is very high:
▪ The heart has a capillary density far exceeding that of skeletal muscle.
▪ Oxygen extraction from arterial blood is very effective within the heart as the resting
myocardium extracts 60%-75% of oxygen from blood.
▪ This amount is higher than that extracted by any other tissue or organ in the body.
▪ As a result, the cardiac venous blood in the coronary sinus, before it reaches the right
atrium and mixes with blood returning from the systemic circulation, is the most
deoxygenated blood in the body.
3. Myocardial oxygen demand and coronary blood flow are tightly coupled:
▪ Because oxygen extraction by the resting heart is already very high, there is little
capacity to increase myocardial oxygen extraction during periods of increased oxygen
demand (eg, during exercise).
▪ Therefore, increased oxygen delivery to the heart can be achieved only through
increased coronary blood flow.
▪ Adenosine and nitric oxide are the most important vasodilators responsible for
increasing coronary flow.
Nitric Oxide
• Synthesized from arginine by nitric oxide synthase.
▪ As a precursor of nitric oxide; arginine supplementation may play an adjunct role in the
treatment of conditions that improve with vasodilation such as stable angina.
• Synthesized by endothelial cells and causes vascular smooth muscle relaxation by a
guanylate cyclase-mediated cGMP second messenger system.
• Nitric oxide Vs. adenosine:
▪ NO → VD on large and pre-arteriolar vessels.
▪ Adenosine → VD on small arterioles.
• NB: Nervous input has very little role on coronary blood flow.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
48. USMLE Endpoint
C V S System
48 Dr/Ahmed Shebl
Autoregulation
• It is the mechanism by which blood flow to each organ remains constant over a wide range of
perfusion pressures.
Pressure-volume Loop & cardiac cycle:
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
49. USMLE Endpoint
C V S System
49 Dr/Ahmed Shebl
UW: ↑ESV→ more volume remaining in the ventricle after contraction.
Pressure-Volume Loop Alterations:
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
50. USMLE Endpoint
C V S System
50 Dr/Ahmed Shebl
• UW: Na nitroprusside: balanced dilator → venodilator (↓preload) & arteriodilator (↓afterload) →
so, SV remain constant.
• UW: furosemide (diuresis) ↓ preload → ↓ EDV.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
51. USMLE Endpoint
C V S System
51 Dr/Ahmed Shebl
• Spinal anesthesia:
▪ ↓ Venous tone → ↓ venous return → ↓ preload.
▪ Has no rule with TPR.
• UW: AV shunt → blood shunts from arterioles (↓afterload) to veins (↑preload).
• UW: Chronic anemia:
▪ ↑ CO → this causes an increase in the slope and height of the cardiac output graph.
▪ ↑ VR due to decreased blood viscosity.
• Rx: ↓Afterload → ↑ SV → ↑ width of the curve.
• Rx: post-radiation therapy → constrictive pericarditis → ↓ EDV.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
52. USMLE Endpoint
C V S System
52 Dr/Ahmed Shebl
LV pressure curve:
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
53. USMLE Endpoint
C V S System
53 Dr/Ahmed Shebl
Starling curve
• Force of contraction is proportional to end-diastolic length of cardiac muscle fiber (preload).
▪ Contractility is increased with catecholamines, positive inotropes.
▪ Contractility is decreased with loss of myocardium (e.g., MI), BB (acutely), non-dihydropyridine
CCBs, dilated cardiomyopathy.
• UW: patient with shock then infused 2L saline → ↑ preload → ↑ end diastolic sarcomere
length.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
54. USMLE Endpoint
C V S System
54 Dr/Ahmed Shebl
Cardiac and vascular function curves:
• Mean Systemic Filling Pressure (MSFP) → Pressure if heart stops.
• UW: which ↑CO & ↑VR with the same MSFP? → ↓TPR (exercise & acute AV shunt)
Which ↑CO & ↑VR with ↑MSFP? → Chronic AV fistula d2 sympathetic and renal
compensation → ↑contractility, ↑vascular tone and ↑blood volume.
Exercise on cardiac and vascular function curves:
• ↑CO & ↑VR & ↓TPR.
• MSFP is constant as MSFP = CO × TPR. (↑CO & ↓TPR)
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
55. USMLE Endpoint
C V S System
55 Dr/Ahmed Shebl
Wigger’s diagram
• UW: dicrotic notch → represents the elasticity of the aorta; lost in AR, Marfan and
syphilis.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
56. USMLE Endpoint
C V S System
56 Dr/Ahmed Shebl
Aortic stenosis
• UW: In aortic stenosis curve: which point corresponds to the maximum point of murmur?
Answer → B. normally, pressure in aorta = pressure in LV during systole.
Mitral stenosis
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
57. USMLE Endpoint
C V S System
57 Dr/Ahmed Shebl
Mitral regurgitation
• V-wave:
▪ LA pressure d2 passive filling during systole.
▪ An abnormally prominent, upsloping left atrial “V wave” during cardiac
catheterization is a major hemodynamic finding of mitral regurge.
Aortic regurgitation
• UW: How to diagnose AR on aortic pressure curve?
1- Absence of diacritic notch.
2- Steep diastolic decline on the curve.
3- High peak of aortic pressure + wide pulse pressure.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
58. USMLE Endpoint
C V S System
58 Dr/Ahmed Shebl
Jugular venous pressure curve:
• Indirectly measures the pressure in the right atrium.
➢ ↑ RAP → ↑JVP: Causes:
▪ Heart failure, fluid overload.
▪ Constrictive pericarditis, cardiac tamponade.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
59. USMLE Endpoint
C V S System
59 Dr/Ahmed Shebl
• A wave—atrial contraction.
▪ Absent in atrial fibrillation (no organized atrial contraction).
▪ Cannon a wave in AV dissociation “complete heart block” → (atria against closed
tricuspid valve).
• C wave—RV contraction (closed tricuspid valve bulging into atrium).
• X descent:
▪ Atrial relaxation and downward displacement of closed tricuspid valve during
ventricular contraction.
▪ Absent in tricuspid regurgitation.
• V wave:
▪ ↑RT atrial pressure due to filling (“villing”) against closed tricuspid valve.
▪ Giant v wave in Tricuspid regurgitation.
• Y descent:
▪ RA emptying into RV.
▪ Rapid deep descent in y-descent → in constrictive pericarditis.
LA pressure curve:
• UW: pt with MS (↑LA pressure on the curve) where is the site of the opening snap?
Answer: C → OS is early diastolic shortly after the aortic component of the second heart sound.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
60. USMLE Endpoint
C V S System
60 Dr/Ahmed Shebl
Heart sounds:
• S1: mitral and tricuspid valve closure. Loudest at mitral area.
• S2: aortic and pulmonary valve closure. Loudest at left upper sternal border.
• S3: in early diastole during rapid ventricular filling phase.
▪ Due to rushing of blood into a partially filled ventricle or very stiff ventricle.
▪ Best heard with:
✓ Bell of the stethoscope pressed lightly over the apex (the bell detects low frequency
voices)
✓ Left lateral decubitus.
✓ At the end of expiration.
• S4:
▪ In late diastole (“atrial kick”).
▪ Left atrium must push against stiff LV wall.
▪ High atrial pressure.
▪ Best heard at apex with patient in left lateral decubitus position.
▪ Associated with ventricular hypertrophy.
• Rx: in aortic stenosis ↑ isovolumetric contraction phase d2 need to ↑ pressure to open the
stenotic valve.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
61. USMLE Endpoint
C V S System
61 Dr/Ahmed Shebl
Splitting
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
62. USMLE Endpoint
C V S System
62 Dr/Ahmed Shebl
Auscultation of the heart
• UW: Left lateral decubitus ↑ intensity of which murmurs? → MS, MR, left sided S3 & S4
• NB: Inspiration → ↑ tricuspid murmurs.
Expiration → ↑ mitral murmurs.
• KQB: Inspiration → ↑ -ve intrathoracic pressure → ↑ venous return → ↑ blood in RV →
pooling of blood of blood in lungs → *↓ systolic arterial pressure.
▪ ↑ HR.
▪ ↓ LV EDP & ↑ RV EDP.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
63. USMLE Endpoint
C V S System
63 Dr/Ahmed Shebl
Valsalva Maneuver
• Bear down as if moving bowels.
• Phase I (few seconds):
➢ ↑ thoracic pressure
➢ ↓ venous return (compression of veins → ↑RA pressure)
➢ Transient rise in aortic pressure (compression)
➢ ↓ heart rate and AV node conduction (baroreceptors)
• Phase II
➢ ↓ Preload → ↓ cardiac output.
➢ ↑ Heart rate and AV node conduction (baroreceptors).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
64. USMLE Endpoint
C V S System
64 Dr/Ahmed Shebl
Heart murmurs:
• Systolic → AS & MR/TR & MVP VSD.
• Diastolic → AR & MS.
• Continuous → PDA.
Systolic murmurs
Aortic stenosis
• Crescendo-decrescendo systolic ejection murmur and soft S2 (ejection click may be
present). Loudest at heart base; radiates to carotids.
• LV >> aortic pressure during systole.
• “Pulsus parvus et tardus”—pulses are weak with a delayed peak.
• Can lead to Syncope, Angina, and Dyspnea on exertion (SAD).
• Most commonly due to age related calcification in older patients (> 60 years old) or in
younger patients with early-onset calcification of bicuspid aortic valve.
• Severe Disease Findings:
➢ Late‐peaking murmur: Slow flow across stenotic valve.
➢ Soft/quiet S2: Stiff valve can’t slam shut.
➢ Pulsus parvus et tardus:
▪ Weak and small carotid pulses
▪ Delayed carotid upstroke
• UW: Aortic stenosis early can cause diastolic dysfunction and hypertrophy then late can
cause systolic dysfunction and LVF.
• UW: patient with AS then developed AF → sudden onset of acute HF (pulmonary edema &
hypotension):
▪ Cause: sudden loss of LV preload.
▪ Explanation: acute AF most likely
precipitated sudden HF in chronic AS as
AF → loss of atrial systolic kick → ↓LV
preload → ↓LVEDV → ↓CO with AS
that caused concentric LV hypertrophy
which worsen the case.
• UW: holosystolic murmurs → MR & TR &
VSD.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
65. USMLE Endpoint
C V S System
65 Dr/Ahmed Shebl
Mitral/tricuspid regurgitation
• Holosystolic, high-pitched “blowing murmur.”
• Mitral: loudest at apex and radiates toward axilla. MR is often due to ischemic heart
disease (post-MI), MVP, LV dilatation.
• Tricuspid: loudest at tricuspid area. TR commonly caused by RV dilatation.
• Rheumatic fever and infective endocarditis can cause either MR or TR.
• In MR, what is the best indicator for severity of the problem?
➢ The presence of audible S3 NOT the holosystolic murmur intensity as the later doesn’t
correlate well with the regurgitant volume but correlate with the effective regurgitant orifice.
NOT S4 as MR+S4 → end stage decompensation of severe MR → LV failure; however,
many patients with severe MR may not have developed LV failure.
• Case: HTN + S3 + holosystolic murmur over the apex but the murmur and the S3
disappeared after diuretics and vasodilators → Dx: Functional MR which caused by either:
➢ Transient hemodynamic factor causing LV dilatation → “Acute LV dilatation can separate
otherwise normal mitral valve”.
➢ OR papillary ms ischemia.
• Forward-to-regurgitant flow ratio:
➢ “In MR, some blood is pumped forward through the aortic valve (forward stroke volume),
while some blood is forced backwards through incompetent valve (regurgitant SV).
➢ Determines left ventricular afterload in patients with mitral regurgitation.
➢ Decreasing afterload will increase forward flow while reducing regurgitant flow.
➢ An increase in left ventricular end diastolic volume can contribute to or worsen mitral
regurgitation when the degree of regurgitation is dependent on left ventncular size (eg, in
dilated cardiomyopathy).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
66. USMLE Endpoint
C V S System
66 Dr/Ahmed Shebl
Mitral valve prolapse
• Late systolic crescendo murmur with midsystolic click (MC; due to sudden tensing
of chordae tendineae).
• Most frequent valvular lesion.
• Best heard over apex.
• Loudest just before S2. Usually benign.
• Can predispose to infective endocarditis.
• Can be caused by myxomatous degeneration (1° or 2° to connective tissue disease such as
Marfan or Ehlers-Danlos syndrome), rheumatic fever, chordae rupture.
Ventricular septal defect
• Holosystolic, harsh-sounding murmur. Loudest at tricuspid area.
Diastolic murmurs
Aortic regurgitation (AR)
• High-pitched “blowing” early diastolic decrescendo murmur.
• Long diastolic murmur, hyperdynamic pulse, and head bobbing when severe and chronic.
• Wide pulse pressure.
• Often due to aortic root dilation, bicuspid aortic valve, endocarditis, rheumatic fever.
• Progresses to left HF.
• Murmur best heard when patient sits up and leans forward? → AR.
• UW: In AR, what maintains CO??
▪ ↑ LV preload
▪ Eccentric LVH
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
67. USMLE Endpoint
C V S System
67 Dr/Ahmed Shebl
Mitral stenosis
• Delayed rumbling mid-to-late diastolic murmur.
• Follows opening snap (OS; due to abrupt halt in leaflet motion in diastole, after rapid
opening due to fusion at leaflet tips).
• ↓ Interval between S2 and OS correlates with ↑ severity: Higher left atrial pressure → ↓
time to opening snap.
• LA >> LV pressure during diastole.
• Often a late (and highly specific) sequela of rheumatic fever.
• Chronic MS can result in LA dilatation → dysphagia/hoarseness via compression of
esophagus/left recurrent laryngeal nerve, respectively.
• UW: in MS the opening snap is best heard at mitral opening in pressure volume curve.
• UW: The best indicator of MS severity → A2 – OS interval → the shorter the interval the
more severe the stenosis.
▪ NOT the rumble → as it depends on the patient anatomy.
▪ NOT the presystolic accentuation → as it indicates LA contraction.
• UW: How to differentiate between OS of MS & splitting of S2?
▪ Splitting → ↑ with inspiration.
▪ OS → ↑ with expiration
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
68. USMLE Endpoint
C V S System
68 Dr/Ahmed Shebl
• UW: in MS → normal LV diastolic pressure. But if MS + ↑ LVEDP → suspect presence of
additional lesion e.g
1. Rheumatic involvement of aortic valve (typically cause combined AR & AS)
2. Infective endocarditis superimposed aortic valve deformity.
• MS + stroke → d2 LA dilatation → atrial mural thrombus.
• MS + TR → d2 ↑ LA pressure → ↑ PCWP → pulmonary HTN → pulmonary vascular
sclerosis → ↓ compliance → RV dilatation → functional TR.
• UW: Late diastolic murmur eliminated by atrial fibrillation → MS & TS.
Continuous murmurs
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
69. USMLE Endpoint
C V S System
69 Dr/Ahmed Shebl
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
70. USMLE Endpoint
C V S System
70 Dr/Ahmed Shebl
Myocardial action potential
• Also occurs in bundle of His and Purkinje fibers.
• Phase 0:
▪ Rapid upstroke and depolarization.
▪ Voltage-gated Na+ channels open.
• Phase 1:
▪ Initial repolarization.
▪ Voltage-gated K+ channels begin to open.
• Phase 2:
▪ Plateau → Ca2+ influx through voltage-gated Ca2+ channels balances K+ efflux.
▪ Ca2+ influx triggers Ca2+ release from sarcoplasmic reticulum and myocyte contraction.
▪ ↓ With CCBs & ↑ with K channel antagonists.
• Phase 3:
▪ Rapid repolarization.
▪ Massive K+ efflux due to opening of voltage-gated slow K+ channels and closure of
voltage-gated Ca2+ channels.
▪ Execution by K infusion → ↑ K in ECF → no K efflux → no repolarization → arrest.
• Phase 4:
▪ Resting potential.
▪ High K+ permeability through K+ channels → constant outward leak of K+.
▪ Na+ and Ca2+ channels are closed.
▪ UW: the resting potential of cardiac ms (phase 4) is -90 not -70, why? → to reduce the
risk for arrhythmia, as larger stimulus is needed to excite the cells.
• In contrast to skeletal muscle:
▪ Cardiac muscle action potential has a plateau, which is due to Ca2+ influx and K+ efflux.
▪ Cardiac muscle contraction requires Ca2+ influx from ECF to induce Ca2+ release from
sarcoplasmic reticulum (Ca2+-induced Ca2+ release).
▪ Cardiac myocytes are electrically coupled to each other by gap junctions.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
71. USMLE Endpoint
C V S System
71 Dr/Ahmed Shebl
Cardiac muscle contraction
• UW: Verapamil is a CCB but doesn’t affect skeletal ms?
▪ Skeletal muscles:
o Doesn’t depend on extracellular calcium → doesn’t require extracellular
calcium influx for excitation contraction coupling.
o Ca comes from SR not from outside.
▪ Cardiac and smooth muscles:
o Depends on extracellular calcium entering by voltage gated L-type calcium
channels for excitation contraction coupling.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
72. USMLE Endpoint
C V S System
72 Dr/Ahmed Shebl
Pacemaker action potential
• Occurs in the SA and AV nodes.
• Key differences from the ventricular action potential include:
1. Phase 0 = upstroke:
▪ Opening of voltage-gated Ca2+ channels.
▪ Fast voltage-gated Na+ channels are permanently inactivated because of the less
negative resting potential of these cells.
▪ Results in a slow conduction velocity that is used by the AV node to prolong
transmission from the atria to ventricles.
2. Phases 1 and 2 are absent.
3. Phase 3 = repolarization:
▪ Inactivation of the Ca2+ channels and ↑ activation of K+ channels → ↑
K+ efflux.
4. Phase 4 (slow spontaneous diastolic depolarization)
▪ Occurs due to:
• Closure of repolarizing K channels.
• Slow influx of Na through funny channels.
• Opening of T-type Ca channels
▪ If channels
• Responsible for a slow, mixed Na+/K+ inward current.
• Different from INa in phase 0 of ventricular action potential.
• Accounts for automaticity of SA and AV nodes.
▪ The slope of phase 4 in the SA node determines HR.
▪ ACh/adenosine ↓ the rate of diastolic depolarization and ↓ HR, while
catecholamines ↑ depolarization and ↑ HR.
▪ Sympathetic stimulation ↑ the chance that If channels are open and thus ↑ HR.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
73. USMLE Endpoint
C V S System
73 Dr/Ahmed Shebl
• Threshold potential:
▪ The amount of depolarization required to initiate the action potential.
▪ Increased by class 1 antiarrhythmic (Na channel blockers) and class 4 (CCBs).
• Role of Verapamil in pacemaker action potential:
▪ Slows diastolic depolarization by ↓ Ca influx during phase 0 and the later part of
phase 4 → ↓ rate of SA node firing and slows AV node conduction.
• Role of Adenosine and acetylcholine in action potential:
▪ Pacemaker cells:
✓ Affect phase 4 of the action potential reducing the rate of spontaneous
depolarization in cardiac pacemaker cells.
✓ Inhibits L-type Ca channels → further prolonging the depolarization time.
✓ These actions result in a transient slowing of the sinus rate and an increase
in AV nodal conduction delay.
✓ Adenosine is useful in the termination of paroxysmal supraventricular
tachycardia.
▪ Myocytes:
✓ Activates potassium channels →↑ K conductance → membrane potential
remains negative for a longer period.
▪ Acetylcholine behaves similarly by increasing outward K. conductance while
decreasing inward Ca and Na currents during phase 4.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
74. USMLE Endpoint
C V S System
74 Dr/Ahmed Shebl
• Norepinephrine & sympathetic on pacemaker action potential:
▪ Opens L-type Ca channel and Na channels in phase 4 → ↓ time taken to reach the
threshold → ↑ automaticity.
• Ivabradine:
▪ Drug that ↓HR without affecting contractility.
✓ As it acts only on phase 4 of the SA node unlike other drugs decreasing HR.
✓ Ivabradine selectively inhibits the funny sodium channels prolonging the slow
depolarization phase (phase 4) and slowing the sinoatrial node firing rate.
▪ It has a negative chronotropic effect with no effect on cardiac contractility
(inotropy) and/or relaxation (lusitropy).
▪ Used in chronic HF with ↓EF and persistent symptoms despite approprtiate ttt.
↓risk of hospitilization d2 HF.
• Inotropic → ↑ contractility → by ↑ inward Ca current.
• Chronotropic → ↑ HR → by ↑ inward Na current→ ↑ SA node firing.
• Dromotropic → ↑ conduction velocity through AV node → by ↑ inward Ca current.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
75. USMLE Endpoint
C V S System
75 Dr/Ahmed Shebl
Pacemakers
• SA node
▪ Dominant pacemaker of the heart.
▪ Located at junction of RA and SVC.
▪ Beats at 60-100 bpm.
• Other pacemakers exist but are slower: If SA node fails, others takeover
▪ AV node (40-60 bpm):
✓ Located in posteroinferior part of interatrial septum.
✓ Blood supply usually from RCA.
✓ 100-msec delay allows time for ventricular filling.
▪ HIS (25-40 bpm)
▪ Bundle branches (25-40 bpm)
▪ Purkinje fibers (25–40 bpm)
Conduction Velocities:
▪ SLOWEST conduction is through AV node.
▪ Very important so ventricle has time to fill.
▪ Purkinje fibers → fastest conduction.
▪ Purkinje > Atria > Vent > AV node.
• Conduction pathway:
▪ SA node → atria → AV node → bundle of His → right
and left bundle branches → Purkinje fibers →
ventricles; left bundle branch divides into left anterior
and posterior fascicles.
• Determining Heart Rate
▪ 3 – 5 big boxes between QRS complex.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
76. USMLE Endpoint
C V S System
76 Dr/Ahmed Shebl
Electrocardiogram
ECG waves
• P wave:
▪ Atrial depolarization. Atrial repolarization is masked by QRS complex.
▪ No p waves:
✓ Irregular rhythm → Atrial fibrillation – irregularly irregular.
✓ Regular rhythm → Hidden p waves: retrograde, Supraventricular tachycardias (SVTs),
Ventricular tachycardia.
▪ P waves present, irregular rhythm:
✓ Sinus rhythm with PACs
✓ Multifocal atrial tachycardia
✓ Sinus with AV block
• PR interval:
▪ Time from start of atrial depolarization to start of ventricular depolarization.
▪ It reflects conduction through the AV node.
▪ Normally < 200 msec.
✓ If > 200 msec. → first degree heart block is said to be present
• QRS complex:
▪ Ventricular depolarization → phase 0 in ventricular contraction (in myocardial action potential
curve).
▪ Normally < 120 msec. Wide QRS > 120 msec → bundle branch block or ventricular tachycardia.
• QT interval:
▪ It represents the time taken for ventricular depolarization and repolarization, effectively the
period of ventricular systole from ventricular isovolumetric contraction to isovolumetric
relaxation (mechanical contraction of the ventricles).
▪ Short Qt: Hypercalcemia.
▪ Prolonged Qt: Hypocalcemia, drugs, LQTS
• T wave:
▪ Ventricular repolarization. T-wave inversion may indicate ischemia or recent MI.
▪ Peaked T waves: ↑ K, Early ischemia (hyperacute).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
77. USMLE Endpoint
C V S System
77 Dr/Ahmed Shebl
• J point:
▪ Junction between end of QRS complex and start of ST segment.
• ST segment:
▪ Isoelectric, ventricles depolarized.
• U wave:
▪ Prominent in hypokalemia (think hyp“U”kalemia), bradycardia.
QRS Axis
• The axis of the heart tends to move
▪ Toward the hypertrophied tissue and
▪ Away from the infarcted tissue
• Rt Axis Deviation → RVH, MI on the Lt and conduction deficit on the Rt.
• Lt Axis Deviation → LVH, MI on the RT and conduction deficit on the Lt.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
78. USMLE Endpoint
C V S System
78 Dr/Ahmed Shebl
Axis Quick Method
• First, glance at aVr → it should be negative.
• If upright, suspect limb lead reversal.
Torsades de pointes
• Torsades de pointes = twisting of the points.
• Polymorphic ventricular tachycardia characterized by shifting sinusoidal waveforms on ECG.
• Can progress to ventricular fibrillation (VF).
• Long QT interval predisposes to torsades de pointes.
• Caused by drugs, ↓ K+, ↓ Mg2+, ↓ Ca+2, congenital abnormalities.
• Treatment includes magnesium sulfate.
Congenital long QT syndrome
• Inherited disorder of myocardial repolarization, typically due to ion channel defects
➢ ↑ Risk of sudden cardiac death due to torsades de pointes.
• Includes:
➢ Romano-Ward syndrome:
▪ Autosomal dominant, pure cardiac phenotype (no deafness).
➢ Jervell and Lange-Nielsen syndrome:
▪ Autosomal recessive, sensorineural deafness.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
79. USMLE Endpoint
C V S System
79 Dr/Ahmed Shebl
Brugada syndrome
• Autosomal dominant disorder most common in Asian males.
• Mutations in the cardiac sodium channel SCN genes.
• ECG pattern of pseudo-right bundle branch block and ST elevations in V1-V3.
• ↑ Risk of ventricular tachyarrhythmias and SCD.
• Prevent SCD with implantable cardioverter-defibrillator (ICD).
• Patients with schizophrenia appear significantly more likely to have Brugada.
Wolff-Parkinson-White syndrome
• Most common type of ventricular preexcitation syndrome.
▪ Abnormal heart rhythm in which the ventricles of the heart become depolarized too early,
which leads to their partial premature contraction
• Abnormal fast accessory conduction pathway from atria to ventricle (bundle of Kent)
bypasses the rate-slowing AV node → ventricles begin to partially depolarize earlier →
characteristic delta wave with widened QRS complex and shortened PR interval on ECG.
• May result in reentry circuit → supraventricular tachycardia.
▪ Recurrent temporary arrhythmia in otherwise normal person → WPW syndrome.
• Don’t slow AV node with (digoxin, CCBs, BBs or adenosine) but block the accessory
pathway with (antiarrhythmic Ia & III).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
80. USMLE Endpoint
C V S System
80 Dr/Ahmed Shebl
Atrial fibrillation
• Chaotic and erratic baseline with no discrete P waves in between irregularly QRS complexes.
• Irregularly irregular heartbeat.
• Risk factors:
✓ Most common risk factors include hypertension and coronary artery disease (CAD).
✓ Occasionally seen after binge drinking ("holiday heart syndrome")
• Can lead to thromboembolic events, particularly stroke.
• Treatment includes anticoagulation, rate control, rhythm control, and/or cardioversion.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
81. USMLE Endpoint
C V S System
81 Dr/Ahmed Shebl
Atrial flutter
• A rapid succession of identical, back-to-back atrial depolarization waves.
• The identical appearance accounts for the "sawtooth" appearance of the flutter waves.
• Treat like atrial fibrillation. Definitive treatment is catheter ablation.
Ventricular fibrillation
• A completely erratic rhythm with no identifiable waves.
• Fatal arrhythmia without immediate CPR and defibrillation.
UW: In AF, which factor determines the ventricular rate?
➢ AV node refractory period.
“ AF occurs due to irregular electrical activity in the atrium; while some of the atrial
impulses are transmitted to the ventricles, most are not due to AV nodal refractory period”
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
82. USMLE Endpoint
C V S System
82 Dr/Ahmed Shebl
AV block
First-degree AV block
• The PR interval is prolonged (> 200 msec).
• Benign and asymptomatic. No treatment required.
Second-degree AV block
1. Mobitz type I (Wenckebach):
a. Progressive lengthening of PR interval until a beat is “dropped” (a P-wave not followed by
a QRS complex).
b. The level of block is usually the AV node.
c. Usually asymptomatic. Variable RR interval with a pattern (regularly irregular).
2. Mobitz type II
a. Dropped beats that are not preceded by a change in the length of the PR interval (as in type I).
b. Due to defect in His-Purkinje system. For this reason, the PR interval is constant as the AV
node is normal.
c. May progress to 3rd-degree block. Often treated with pacemaker.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
83. USMLE Endpoint
C V S System
83 Dr/Ahmed Shebl
Third-degree (complete) AV block
• Pathophysiology:
➢ Conduction between the SA and AV nodes is impaired → AV nodal cells become
pacemakers → SA node impulses cause atrial contraction while impulses generated
by the AV node cause ventricular contraction.
➢ The ventricular pacing is coming from AV node which becomes the pacemaker.
• ECG:
➢ AV dissociation: the atria and ventricles depolarize independently of each other →
P waves and QRS complexes not rhythmically associated
➢ QRS complexes are narrow since ventricular depolarization proceeds normally.
➢ The AV node produces a heart rate of 45-55 beats per minute.
• Usually treated with pacemaker.
• Can be caused by Lyme disease.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
84. USMLE Endpoint
C V S System
84 Dr/Ahmed Shebl
Bundle branches block
• Both bundle branches blocked → results in AV block; form of HIS-Purkinje system disease.
• ONE bundle branch blocked:
➢ Does not cause AV block
➢ Normal PR interval
➢ QRS will be prolonged
• Symptoms: None
➢ Identified incidentally on ECG
• May progress to AV block (need for pacemaker)
➢ Interfere with detection of ischemia
➢ ST elevations, T-wave inversions can be normal.
• Causes:
➢ Often caused by slowly progressive fibrosis/sclerosis
➢ More common in older patients
➢ Can result from “structural heart disease”
➢ LBBB: Prior MI, cardiomyopathy
➢ RBBB: Right heart failure
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
85. USMLE Endpoint
C V S System
85 Dr/Ahmed Shebl
Right Bundle Branch Block
Left bundle branch block
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
86. USMLE Endpoint
C V S System
86 Dr/Ahmed Shebl
Atrial natriuretic peptide & brain natriuretic peptide
Atrial natriuretic peptide
• Released from atrial myocytes in response to → blood volume and atrial pressure.
• Acts via cGMP.
• Mechanism of action:
1. Kidney:
▪ Dilate afferent and constricts efferent, ↓ Na reabsorption, ↓ renin → diuresis.
▪ Contributing to “aldosterone escape” mechanism.
2. Adrenal gland → ↓ aldosterone.
3. Blood vessels → VD, ↑ capillary permeability.
B-type (brain) natriuretic peptide
• Released from ventricular myocytes in response to ↑ tension.
• Similar physiologic action to ANP, with longer half-life.
• BNP blood test used for diagnosing HF (very good negative predictive value).
• Available in recombinant form (nesiritide) for treatment of HF.
• UW: Neprilysin
▪ Cleaves and inactivates endogenous peptides including natriuretic peptides (eg.
BNP), glucagon, oxytocin and bradykinin.
▪ Inhibition of neprilysin e.g., sacubitril leads to increased levels of endogenous
natriuretic peptides, which promote beneficial effects in heart failure.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
87. USMLE Endpoint
C V S System
87 Dr/Ahmed Shebl
Normal cardiac pressures
• Right-sided pressures in the heart are lower than left-sided pressures due to lower resistance
in the pulmonary vasculature.
• Pulmonary capillary wedge pressure (PCWP)
▪ Good approximation of the left atrial pressure.
▪ PCWP= LA EDP = LV EDP
▪ In mitral stenosis, PCWP > LV EDP.
▪ PCWP is measured by Swan-Ganz catheter.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
88. USMLE Endpoint
C V S System
88 Dr/Ahmed Shebl
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
89. USMLE Endpoint
C V S System
89 Dr/Ahmed Shebl
Exercise physiology
Capillary fluid exchange
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
90. USMLE Endpoint
C V S System
90 Dr/Ahmed Shebl
• UW: Venous thrombosis is causing edema just like CHF → causes edema by ↑ capillary
hydrostatic pressure.
• UW: patient e CHF and ↑ CVP but there is no edema! Why? → D2 ↑ tissue lymphatic drainage
which can compensate for moderate CVP elevation to prevent development of clinically apparent
edema.
3rd Spacing
• Intracellular fluid – 1st space → About 2/3 body fluid.
• Extracellular fluid – 2nd space → About 1/3 body fluid.
• Third spacing - fluid where it should NOT be:
✓ Pleural effusions, Ascites, Cerebral edema.
• Low intravascular volume/High total volume
• Occurs post-op, sepsis.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
91. USMLE Endpoint
C V S System
91 Dr/Ahmed Shebl
CVS PATHOLOGY
Hypertension
• Defined as persistent systolic BP ≥ 140 mm Hg and/or diastolic BP ≥ 90 mm Hg.
PRIMARY HTN:
• HTN of unknown etiology (90% of cases). Related to ↑ CO or ↑ TPR.
• Risk factors: Age, obesity, diabetes, physical inactivity, excess salt intake, excess alcohol
intake, cigarette smoking, family history; African American > Caucasian > Asian.
Secondary HTN:
• HTN due to an identifiable etiology (10% of cases).
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
92. USMLE Endpoint
C V S System
92 Dr/Ahmed Shebl
Renal artery stenosis
Fibromuscular dysplasia
• Physical examination:
• Hum or bruit in costovertebral angle due to well-developed
collaterals.
• Right renal is more affected than left → renin and angiotensin
↑ (2° hyperaldosteronism).
• Carotid bruit can also be heard
• Angiography: “string of beads” pattern to renal artery.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
93. USMLE Endpoint
C V S System
93 Dr/Ahmed Shebl
Hypertensive crisis
Hypertension complications:
• CAD, LVH, HF, atrial fibrillation; aortic dissection, aortic aneurysm; stroke; chronic kidney
disease (hypertensive nephropathy); retinopathy.
Hyperlipidemia signs
• Xanthomas:
▪ Plaques or nodules composed of lipid-laden histiocytes in skin A, especially the eyelids
(xanthelasma B).
▪ Lipid laden histiocytes: dermal accumulation of macrophages containing cholesterol
and triglycerides.
• Tendinous xanthoma:
▪ Lipid deposit in tendon C, especially Achilles.
• Corneal arcus:
▪ Lipid deposit in cornea.
▪ Common in elderly (arcus senilis D), but appears earlier in life with hypercholesterolemia
• Familial hypercholesterolemia:
▪ One of the most common autosomal dominant disorders.
▪ Cause: mutation in the LDL receptor gene in the liver which clears 70% of the LDL in
the blood → accelerated atherosclerosis → early onset coronary artery disease.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
94. USMLE Endpoint
C V S System
94 Dr/Ahmed Shebl
Arterioscelorosis
• Literally, "hard arteries;" due to thickening of the blood vessel wall.
• Three pathologic patterns:- atherosclerosis, arteriolosclerosis, and Monckeberg medial calcific
sclerosis.
1- ARTERIOLOSCLEROSIS
• Narrowing of small arterioles; divided into hyaline and hyperplastic types.
Hyaline arteriolosclerosis
• Caused by proteins leaking into the vessel wall, producing vascular thickening; proteins are seen
as pink hyaline on microscopy.
• Consequence of long-standing benign hypertension or diabetes.
• Results in reduced vessel caliber with end-organ ischemia; classically produces glomerular
scarring (arteriolonephrosclerosis) that slowly progresses to chronic renal failure.
Hyperplastic arteriolosclerosis
• Involves thickening of vessel wall by hyperplasia of smooth muscle ('onion-skin' appearance).
• Consequence of malignant hypertension.
• Results in reduced vessel caliber with end-organ ischemia.
• May lead to fibrinoid necrosis of the vessel wall with hemorrhage; classically causes acute
renal failure with a characteristic 'flea-bitten' appearance.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
95. USMLE Endpoint
C V S System
95 Dr/Ahmed Shebl
2- MONCKEBERG MEDIAL CALCIFIC SCLEROSIS
• Calcification of the media of muscular (medium-sized) arteries; nonobstructive.
• Not clinically significant; seen as an incidental finding on x-ray or mammography.
3- Atherosclerosis
• Plaque accumulation in arterial walls.
• Chronic inflammatory process; involves macrophages, T-cells.
• Form of arteriolosclerosis caused by accumulation of lipoproteins especially LDL.
• Underlying cause of many diseases: • Myocardial infarction • Stroke • Peripheral vascular disease
• Affected arteries:
➢ Large elastic arteries: Aorta, carotid arteries, iliac arteries.
➢ Medium‐sized muscular arteries: Coronary, popliteal
(Abdominal aorta > coronary artery > popliteal > carotid artery.)
• Risk factors:
➢ Modifiable: smoking, hypertension, hyperlipidemia (↑LDL), diabetes.
➢ Nonmodifiable: age, sex (more in men and postmenopausal women), family history.
• Pathophysiology:
➢ Endothelial injury or dysfunction:
▪ Details incompletely understood; believed to be related to risk factors.
▪ Cigarette smoke, high blood pressure, high cholesterol.
▪ Common sites for plaques are branch points and vessel origins (ostia).
➢ Lipids:
▪ LDL accumulation in intima → Oxidized by free radicals.
▪ Oxidized LDL scavenged by macrophages → Cannot be degraded.
▪ Macrophages become foam cells → fatty streaks.
➢ Chronic inflammation:
▪ LDL oxidized from free radicals damages endothelium, smooth muscle.
▪ Macrophages release cytokines → smooth muscle migration.
➢ Smooth muscle cells:
▪ Proliferate in intima → lay down extracellular matrix → fibrous plaques.
▪ Key growth factor: Platelet-derived growth factor “PDFG”.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
96. USMLE Endpoint
C V S System
96 Dr/Ahmed Shebl
• Atheroma Growth:
➢ Fatty streaks:
▪ Macrophages filled with lipids.
▪ Form line (steak) along vessel lumen → Do not impair blood flow.
▪ Can be seen in children, adolescents.
▪ Not all progress.
➢ Atherosclerotic plaques
▪ Intima thickens, lipids accumulate.
▪ Usually patchy along vessel wall; rarely involve entire vessel wall.
▪ Usually eccentric.
UW: Vascular smooth muscle cells are the only cells within the atherosclerotic plaque capable of
synthesizing structurally important collagen and other matrix components. Progressive enlargement
of the plaque results in remodeling of the extracellular matrix and VSMC death, promoting
development of vulnerable plaques with an increased propensity for rupture.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
97. USMLE Endpoint
C V S System
97 Dr/Ahmed Shebl
Atherosclerosis Complications
• Ischemia.
• Plaque rupture:
➢ Exposes thrombogenic substance → clot formation.
➢ May cause acute vessel closure (STEMI)
➢ Thrombus may embolize (stroke from carotid plaque)
• Hemorrhage into plaque:
➢ Lesions in intima causes proliferating small vessels (“neovascularization”)
➢ Contained rupture may suddenly expand lesion.
• Aneurysm:
➢ Lesions may damage underlying media.
➢ Plaque associated with abdominal aortic aneurysms.
• Dystrophic Calcification
➢ Commonly seen in atheroma.
➢ Result of chronic inflammation.
➢ Basis for “coronary CT scans”
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
98. USMLE Endpoint
C V S System
98 Dr/Ahmed Shebl
UW: Case Scenario: 12y + flat yellow spots on the inner surface of the aorta.
❖ Fatty streaks:
▪ Not raised, don’t disturb blood flow and shows intracellular lipid accumulation.
▪ Presents in all aortas of all children > 10 years → normal finding.
UW: Which cell does provide the major proliferative stimuli for cellular component of the
atherosclerotic plaques?
❖ PLATELETS:
▪ Endothelial injury → platelet adhesion.
▪ PDGF→ smooth ms migration from media to intima and proliferation.
▪ TGF→ interstitial collagen production.
UW: Vascular reaction to intimal injury → intimal hyperplasia and fibrosis → mediated by
smooth ms cells that migrate from the media to the intima.
▪ Fibrous plaque = intimal plaque = necrotic lipid core + fibromuscular cap.
UW: Prostacyclin (Prostaglandin I2)
▪ Synthesized by prostacyclin synthase in the capillary endothelium.
▪ Function:
1. Inhibits platelet aggregation and adhesion
2. Vasodilates and increases vascular permeability and stimulates leukocyte
chemotaxis.
▪ Normally, prostacyclin exists in dynamic balance with thromboxane A2 (TXA2), a
prostaglandin that enhances platelet aggregation and causes vasoconstriction.
▪ Prostacyclin and TXA2 together maintain capillary patency and normal blood flow.
▪ Damaged endothelial cells lose the ability to synthesize prostacyclin, and therefore
predispose to the development of thrombi and hemostasis. Synthetic prostacyclin is
used in the treatment of pulmonary hypertension peripheral vascular disease and
Raynaud syndrome.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
99. USMLE Endpoint
C V S System
99 Dr/Ahmed Shebl
Aortic aneurism
• Localized pathologic dilatation of the aorta.
THORACIC ANEURYSM
• Due to weakness in the aortic wall.
• Risk factors include:
1. Hypertension.
2. Connective tissue disease (eg, Marfan syndrome) due to cystic medial degeneration:
Myxomatous changes in the media of the arteries.
3. Bicuspid aortic valve
4. 3° syphilis (obliterative endarteritis of the vasa vasorum)
▪ Results in a 'tree-bark' appearance of the aorta.
• Major complications:
1. Dilation of the aortic valve root, resulting in aortic valve insufficiency
2. Compression of mediastinal structures (e.g., airway or esophagus)
3. Thrombosis/embolism.
ABDOMINAL AORTIC ANEURYSM
• Usually arises below the renal arteries, but above the aortic bifurcation.
• Primarily due to atherosclerosis; classically seen in male smokers> 60 years old with HTN.
1. Atherosclerosis increases the diffusion barrier to the media, resulting in atrophy and
weakness of the vessel wall.
• Presents as a pulsatile abdominal mass that grows with time.
• Major complication is rupture, especially when > 5 cm in diameter; presents with triad of
hypotension, pulsatile abdominal mass, and flank pain.
1. Other complications include compression of local structures (e.g., ureter) and
thrombosis/embolism.
UW: Direct cause of AAA → transmural inflammation of the aortic wall.
Although atherosclerotic changes are frequently present in patients with AAA, these are limited
to the inner aortic wall layers. In contrast, AAAs are characterized by transmural inflammation of
the aortic wall. Chronic inflammation leads to degradation of elastin and collagen by proteases,
resulting in loss of elastin and smooth muscle cells and abnormal collagen remodeling and cross-
linking. These changes lead to weakening and progressive expansion of the aortic wall resulting
in aneurysm formation.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
100. USMLE Endpoint
C V S System
100 Dr/Ahmed Shebl
Aortic dissection
• Longitudinal intimal tear forming a false lumen.
• Occurs in the proximal 10 cm of the aorta (high stress region) with preexisting weakness of the
media.
• Most common cause is hypertension (older adults); also associated with inherited defects of
connective tissue (younger individuals)
1. Hypertension
▪ Single most important risk factor.
▪ Results in hyaline arteriosclerosis of the vasa vasorum; decreased flow causes
atrophy of the media.
2. Marfan syndrome and Ehlers-Danlos syndrome classically lead to weakness of
the connective tissue in the media (cystic medial necrosis).
• Presents as sharp, tearing chest pain that radiates to the back +/- markedly unequal BP in
arms. CXR → mediastinal widening.
• Complications include pericardial tamponade (most common cause of death), rupture with fatal
hemorrhage, and obstruction of branching arteries (e.g., coronary or renal) with resultant end-
organ ischemia.
Stanford classification of aortic dissection
• Stanford type A refers to aortic dissections that involve any part of the ascending aorta.
▪ Usually originate in the sinotubular junction.
▪ The areas are thought to be predominantly affected due to increases in the rate of rise
of pressure and in shearing forces at these sites in patients with severe hypertension.
• Stanford type B refers to all other dissections involving the descending aorta.
▪ Typically originate close to the origin of the left subclavian artery.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
101. USMLE Endpoint
C V S System
101 Dr/Ahmed Shebl
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
102. USMLE Endpoint
C V S System
102 Dr/Ahmed Shebl
Cardiac ischemia
• The likelihood of MI is increased with the action of metalloproteinase → degrade collagen
→ ↓ plaque stability → plaque rupture.
Stable Angina
• Angina: Chest pain due to ischemic myocardium secondary to coronary artery narrowing or
spasm; no myocyte necrosis.
• Results from myocardial oxygen demand-supply mismatch.
• Manifests as chest pressure, tightness, or pain that is reliably produced by exertion and
relieved by rest or nitroglycerin.
• Occurs due to a fixed atherosclerotic plaque obstructing >70% of the coronary artery
lumen that limits blood flow during exertion.
• Stable (fixed) atherosclerotic plaque characteristics:
▪ No plaque ulceration
▪ No thrombus
▪ Usually with ST depression on ECG.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
103. USMLE Endpoint
C V S System
103 Dr/Ahmed Shebl
Acute Coronary Syndromes
• Unstable atheromatous plaque → plaque rupture → thrombus formation.
▪ Subtotal occlusion:
▪ Unstable angina
▪ Non-ST elevation myocardial infarction
▪ Total occlusion (100%):
▪ ST-elevation myocardial infarction (STEMI)
• Characters of unstable atheromatous plaque:
✓ Thin fibrous cap → ulcerate → rupture → thrombosis → MI.
▪ Activated macrophages in atheroma → metalloproteinase → collagen
degradation → intimal inflammation → ulceration.
▪ STATINS decrease this inflammation and are useful in ACS to stabilize the plaque.
✓ Rich lipid core → rupture.
Unstable angina
• Thrombosis with incomplete coronary artery occlusion.
• +/- ST depression and/or T-wave inversion on ECG.
• No cardiac biomarker elevation (unlike NSTEMI).
• ↑ in frequency or intensity of chest pain or any chest pain at rest.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
104. USMLE Endpoint
C V S System
104 Dr/Ahmed Shebl
Extent of Ischemia
• Transmural ischemia:
✓ Occurs with complete 100% flow obstruction (STEMI)
• Subendocardial ischemia:
✓ Occurs with flow obstruction but some distal blood flow.
✓ Stable angina, unstable angina, NSTEMI
Vasospastic angina (also known as Prinzmetal or Variant)
• Occurs at rest 2° to coronary artery spasm.
▪ Midnight to early morning.
▪ Sometimes symptoms improve with exertion
• Smoking is a risk factor; hypertension and hypercholesterolemia are not.
• Triggers include cocaine, alcohol, and triptans.
• Transient ST elevation on ECG. Normal cardiac enzymes. Ergonavine provocative test.
• Treat with Ca2+ channel blockers, nitrates, and smoking cessation (if applicable).
• Avoid propranolol (nonselective blocker) → can cause unopposed alpha stimulation →
Symptoms may worsen.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
105. USMLE Endpoint
C V S System
105 Dr/Ahmed Shebl
Coronary steal syndrome
• Distal to coronary stenosis, vessels are maximally dilated at baseline.
• Administration of vasodilators (eg, dipyridamole, regadenoson) dilates normal vessels →
blood is shunted toward well-perfused areas → ischemia in myocardium perfused by
stenosed vessels.
• Principle behind pharmacologic stress tests with coronary vasodilators.
Sudden cardiac death
• Death from cardiac causes within 1 hour of onset of symptoms.
• Most commonly due to a lethal arrhythmia (eg, VF) which is associated with:
➢ CAD (up to 70% of cases)
➢ Cardiomyopathy (hypertrophic, dilated).
➢ Hereditary ion channelopathies (eg, long QT syndrome, Brugada syndrome).
• Prevent with implantable cardioverter defibrillator (ICD).
Myocardial infarction
• Most often due to rupture of coronary artery atherosclerotic plaque → acute thrombosis.
• ↑ Cardiac biomarkers (CK-MB, troponins) are diagnostic.
• Commonly occluded coronary arteries: LAD > RCA > circumflex.
• Symptoms: diaphoresis, nausea, vomiting, severe retrosternal pain, pain in left arm and/or
jaw, shortness of breath, fatigue.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
106. USMLE Endpoint
C V S System
106 Dr/Ahmed Shebl
• How much time does it take for the cardiac muscle to stop after the onset of total
ischemia? → 1 min.
➢ If restoration of blood < 30 min → reversible contractile dysfunction (myocardial
stunning)→ contractility gradually returning to normal over hours to days.
➢ IF restoration > 30 min → total ischemia becomes irreversible.
• Cytoplasmic hypereosinophilia is one of the earliest signs of coagulative necrosis of
myocytes.
• Neutrophils activation → fibrinous pericarditis:
1. Sharp pain increase with coughing, swallowing (d2 irritation of the posterior
pericardium).
2. Radiating to the neck (d2 irritation of the inferior pericardium to the phrenic nerve).
• Macrophages activation → phagocytosis → rupture of:
1. Free wall → cardiac tamponade.
2. Interventricular septum → VSD or shunt.
▪ Holosystolic murmur at the left sternal border 3-10 days post MI.
3. Papillary muscle → mitral regurgitation.
▪ Holosystolic murmur at the apex radiating to the axilla 3-10 days post MI.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
107. USMLE Endpoint
C V S System
107 Dr/Ahmed Shebl
Evolution of myocardial infarction
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
108. USMLE Endpoint
C V S System
108 Dr/Ahmed Shebl
Reversible injuries in cardiac muscle
1. Myofibril relaxation→ early sign < 30 min, due to anaerobic glycolysis.
2. Disaggregation of polysomes → dissociation of rRNA from mRNA→↓protein
synthesis.
3. Disaggregation of nucleus.
4. Clumping of nuclear chromatin d2 ↓PH.
5. Triglyceride droplet accumulation d2 ↓ lipoproteins.
6. Glycogen loss→ early due to ↓ ATP.
• Mitochondrial
1. Swelling → reversible d2 ↓ATP → ↓pumps → ↑ intracellular Na & Ca.
2. Vacuolization → irreversible cell injury which indicates that the mitochondria is
permanently unable to reduce ATP.
• Contraction bands:
▪ Located at the margins of the necrotic area.
▪ Caused by reperfusion of the irreversibly damaged cells → Ca influx →
hypercontraction of the myofibrils.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
109. USMLE Endpoint
C V S System
109 Dr/Ahmed Shebl
Post-infarction ventricular remodeling
• Remodeling is defined as alteration in the structure (dimensions, mass, shape) of the heart in
response to hemodynamic load and/or cardiac injury in association with neurohormonal
activation.
• Following myocardial infarction, stretched infarcted tissue increases left ventricular volume
leading to combined volume and pressure load on noninfarcted zones and
mixed concentric/eccentric hypertrophy.
• An increase in end-diastolic volume occurs early in MI to accommodate a larger preload and
compensate for the acute decrease in contractility after MI.
• Area of infarction → expansion, thinning and regional dysfunction.
• The rest → hypertrophy to compensate.
• Net result → dilated ventricular hypertrophy with enlarged LV cavity.
• Can be prevented by ACEIs or some BB.
Diagnosis of myocardial infarction
• ECG:
▪ The gold standard for MI diagnosis in the first 6 hours.
▪ ECG changes can include
➢ ST elevation (STEMI, transmural infarct), ST depression (NSTEMI,
subendocardial infarct).
➢ Hyperacute (peaked) T waves, T-wave inversion.
➢ New left bundle branch block, and pathologic Q waves or poor R wave
progression (evolving or old transmural infarct).
• Cardiac enzymes:
▪ Cardiac troponin I
➢ Rises after 4 hours (peaks at 24 hr) and is ↑ for 7- 10 days.
➢ More specific than other protein markers.
▪ CK-MB
➢ Rises after 6- 12 hours (peaks at 16- 24 hr)
➢ Predominantly found in myocardium but can also be
released from skeletal muscle.
➢ Useful in diagnosing reinfarction following acute Ml
because levels return to normal after 48 hours.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
110. USMLE Endpoint
C V S System
110 Dr/Ahmed Shebl
ECG localization with STEMI
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
111. USMLE Endpoint
C V S System
111 Dr/Ahmed Shebl
• UW: DM increases the risk of MI by 3 times.
Complications of myocardial infarction
• Cardiac arrhythmia:
▪ Occurs within the first few days after MI.
▪ Important cause of death before reaching the hospital and within the first 24 hours
post-MI.
• Postinfarction fibrinous pericarditis:
▪ Occurs 1–3 days after MI.
▪ Friction rub.
• Papillary muscle rupture:
▪ Occurs 2–7 days after MI.
▪ Posteromedial papillary muscle more common to rupture due to single blood supply
from posterior descending artery.
▪ Can result in severe mitral regurgitation.
▪ Other causes of papillary rupture → bacterial endocarditis (most common cause)
• Interventricular septal rupture:
▪ Occurs 3–5 days after MI.
▪ Macrophage-mediated degradation → VSD → ↑ O2 saturation and pressure in RV.
• Ventricular pseudoaneurysm formation:
▪ Occurs 3–14 days after MI. Contained free wall rupture; ↓ CO, risk of arrhythmia,
embolus from mural thrombus.
• Ventricular free wall rupture:
▪ Occurs 5–14 days after MI. Free wall rupture → cardiac tamponade.
▪ LV hypertrophy and previous MI protect against free wall rupture.
▪ Acute form usually leads to sudden death.
• True ventricular aneurysm:
▪ Occurs 2 weeks to several months after MI.
▪ Outward bulge with contraction (“dyskinesia”), associated with fibrosis.
• Dressler syndrome:
▪ Occurs several weeks after MI.
▪ Autoimmune phenomenon resulting in fibrinous pericarditis.
• LV failure and pulmonary edema:
▪ Can occur 2° to LV infarction, VSD, free wall rupture, papillary muscle rupture with
mitral regurgitation.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
112. USMLE Endpoint
C V S System
112 Dr/Ahmed Shebl
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
113. USMLE Endpoint
C V S System
113 Dr/Ahmed Shebl
UW: SLE may cause an acute coronary syndrome at a young age even with angiographically
normal coronary arteries.
Special complications with MI
Inferior MI
• Right ventricular infarction → loss of right ventricular contractility.
▪ Elevated jugular venous pressure with clear lungs.
▪ Decreased preload to left ventricle → hypotension.
• Sinus bradycardia and heart block
• Hemodynamics:
▪ ↑ Right atrial pressure and CVP.
▪ ↓ CO and pulmonary capillary wedge pressure.
• Diagnosis: Right sided chest leads.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
114. USMLE Endpoint
C V S System
114 Dr/Ahmed Shebl
Left main
• ST‐elevation aVR.
• Diffuse ST depressions.
Chronic myocardial ischemia
1- Hypernating myocardium
• State of chronic myocardial ischemia in which both myocardial metabolism and function are
reduced to match a concomitant reduction in coronary blood flow.
• Due to moderate/severe flow-limiting stenosis.
• This new equilibrium prevents myocardial necrosis.
• Chronically hibernating myocardium demonstrates:
1. ↓ Expression and disorganization of contractile and cytoskeletal proteins.
2. Altered adrenergic control, and reduced calcium responsiveness.
• Mechanism:
1. ↓Energy metabolism but there is sufficient ATP to prevent contracture.
2. ↑gene expression of TNF-alpha and nitric oxide synthase → inhibitors of contracture.
• These changes lead to decreased contractility and left ventricular systolic dysfunction.
• However, coronary revascularization and subsequent restoration of blood flow to
hibernating myocardium improves contractility and LV function.
2- Ischemic preconditioning
• A phenomenon in which brief repetitive episodes of myocardial ischemia followed by
reperfusion, protect the myocardium from subsequent prolonged episodes of ischemia.
• In clinical terms, repetitive episodes of angina prior to myocardial infarction can delay cell
death after complete coronary occlusion and therefore provide greater time for myocardial
salvage with coronary revascularization.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
115. USMLE Endpoint
C V S System
115 Dr/Ahmed Shebl
3- Myocardial STUNNING:
• Less severe form of ischaemia-induced reversible loss of contractile function.
• Cause: brief ischemic episode (<30 min) followed by reperfusion.
• Repetitive stunning can lead to hibernation.
Differential diagnosis of chest pain
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
116. USMLE Endpoint
C V S System
116 Dr/Ahmed Shebl
Peripheral vascular disease
• Intermittent claudication: muscle pain, which occurs with exercise and remits with rest.
• Thigh claudication:
▪ Suggestive of occlusive disease of the ipsilateral external iliac artery or its more
distal branches (eg, common femoral, superficial femoral, profunda femoris arteries).
▪ Accompanying impotence and/or gluteal claudication suggests more proximal
aortoiliac occlusion (so-called Leriche syndrome), which, in addition to affecting
the external iliac artery, also diminishes blood flow to the internal pudendal and
gluteal branches of the internal iliac artery.
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint
117. USMLE Endpoint
C V S System
117 Dr/Ahmed Shebl
Cardiomyopathies
Dilated cardiomyopathy
• Dilation of all four chambers of the heart. Most common cardiomyopathy (90% of cases).
• Causes:
▪ Often idiopathic or familial (Genetic mutation → usually autosomal dominant mutation
in dystrophin gene).
▪ Other etiologies include chronic Alcohol abuse, wet Beriberi, Coxsackie B viral
myocarditis, chronic Cocaine use, Chagas disease, Doxorubicin toxicity,
hemochromatosis, sarcoidosis, thyrotoxicosis, peripartum cardiomyopathy.
• Findings:
▪ HF (eccentric hypertrophy, systolic dysfunction, S3).
▪ Systolic regurgitant murmur.
▪ CXR: balloon appearance of heart.
▪ Echo: dilatation of all chambers & biventricular failure.
• Treatment:
▪ Na+ restriction, ACE inhibitors, β-blockers, diuretics, digoxin, ICD, heart transplant.
• Doxorubicin DCM:
✓ Cumulative dose dependent → presents many months after discontinuation of the drug.
✓ Prevented by → DEXRAZOXANE: iron chelating agent that ↓ O2 free radicals
produced by doxorubicin.
Dystrophin: which normally links the internal myocyte cytoskeleton with the external basement
membrane (Remember that dystrophin mutations are also found in the common skeletal
myopathies, i.e., Duchenne and Becker muscular dystrophies.)
https://t.me/USMLEEndopoint
https://t.me/USMLEEndopoint