Ebsteins anomaly dr hafeesh fazulu
•Download as PPTX, PDF•
4 likes•208 views

This document provides an overview of Ebstein's anomaly, a congenital heart defect characterized by abnormal attachment of the tricuspid valve leaflets to the myocardium. It discusses the history and typical features of the condition, including displaced valve leaflets, enlargement of the right ventricle and atrium, and arrhythmias. The document outlines evaluation with echocardiogram, ECG and chest x-ray, and indicates interventions like tricuspid valve repair are recommended for those with cyanosis, heart failure or decreased functional capacity. While neonatal Ebstein's carries a poor prognosis, satisfactory valve repair can result in good medium and long-term outcomes.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ebsteins anomaly dr hafeesh fazulu
Similar to Ebsteins anomaly dr hafeesh fazulu (20)
More from Hafeesh Fazulu
More from Hafeesh Fazulu (12)
Recently uploaded
Recently uploaded (20)
Ebsteins anomaly dr hafeesh fazulu
- 1. EBSTEINS ANOMALY Dr Hafeesh Fazulu DM Resident
- 2. HISTORY • 1866 – Autopsy Report by Wilhelm Ebstein reported a strikingly ABNORMAL Tricuspid valve • Anterior leaflet – normal • But SEPTAL & INFERIOR leaflets were abnormal • 1950 – clinically recognised.
- 4. • Normal tricuspid leaflets consist of basal attachments to the annulus (right atrioventricular sulcus), peripheral zones into which chordae tendineae insert, and clear zones that lie between the basal attachments and the peripheral zones. • The semicircular or quadrangular anterior leaflet is the largest of the three. • The posterior leaflet is scalloped.
- 5. • The septal leaflet attaches chiefly to the ventricular septum , but part of its basal attachment is to the posteriorwall of the right ventricle. • The septal leaflet normally exhibits a slight but distinct apical displacement of its basal attachment compared with the mitral valve
- 6. MORPHOLOGY in EBSTEINS 1. Adherence of the septal and inferior leaflets to the underlying myocardium. 2. Downward displacement of the functional annulus. 3. Dilation of the “atrialized” portion of the RV, with variable degrees of thinning of the free wall. 4. Redundancy, fenestrations and tethering of the anterior leaflet. 5. Dilation of the right AV junction (true tricuspid annulus).
- 11. EPIDEMOLOGY • 0.3-0.8% of all congenital heart diseases. • 1 in 20,000-50,000 live births. • Equal male: female occurrence. • The relative risk of Ebstein’s anomaly is increased by 500-fold in offspring exposed to in utero lithium carbonate (Danish registery). • Mortality in the neonatal period is 20%-40%. and less than 50% survive to 5 years. • Mortality at all ages is 12.5%
- 12. • ASD/PFO in 80-94% • Additional associated anomalies : VSD +/- pulmonary atresia RVOT obstruction PDA Coarctation • Left sided lesions in 39%: MVP, systolic dysfunction, Subaorticstenosis, BAV, LV muscle bands, LV noncompaction in 18%. • Accessory conduction pathway in 15-20%, usually near the orifice of TV. • CCTGA (15-50% of CCTGA patients meet criteria for EA).
- 13. ETIOLOGY & GENETIC FACTORS • More common in twins. • Family history of congenital heart disease • Maternal exposure to benzodiazepines. • Maternal lithium therapy. • Most cases are sporadic. • Familial Ebstein’s anomaly is rare.
- 14. Genetic factors • Rare cases of cardiac transcription factor NKX2.5 mutations, • 10p13-p14 deletion, 1p34.3-p36.11 deletion have been described in the anomaly .
- 15. NATURAL HISTORY • Depends on severity • When valve deformity is extreme – death in utero • Severe – Symtoms in Neonate • Moderate – Symtoms in Adolescence or young adult • Mild – survival to 9th decade reported.
- 16. CLINICAL RECOGNITION • 1994 Study Celermajer et al – 60% recognised before age 1 • 10% are undiagnosed into adulthood
- 17. CLINICAL FEATURES • Most common presentation by age: • Fetus: abnormal routine scan (86%) • Neonates: cyanosis (74%) • Infants: heart failure (43%) • Children: Incidental murmur (63%) • Teens and adults: arrhythmia (42%), decreased exercise tolerance, fatigue, right-sided failure, paradoxical embolism, brain abscess.
- 18. Physical Examination • Cyanosis - Varying degrees of cyanosis at various times in life and transient worsening with arrhythmias. • Precordial asymmetry • Usually left parasternal prominence and occasionally right parasternal prominence. • Absent left parasternal (ie, right ventricular) lift an important negative sign.
- 19. • Arterial pulses • Usually normal • Diminished volume • Heart sounds • First heart sound • widely split with loud tricuspid component( THE SAIL SOUND ) • Mitral component - soft (long PR interval) • Second heart sound • usually is normal • widely split when the pulmonary component is delayed due to RBBB.
- 20. • Additional heart sounds and murmurs • Third and fourth heart sounds • commonly present.(QUADRUPLE RHYTHM) • Summation of third and fourth heart sounds, especially with prolonged PR interval, can mimic an early diastolic murmur. • The systolic murmur of tricuspid regurgitation • Medium frequency and decrescendo in nature (grade2/6 or 3/6). • At the lower left parasternal area and sometimes at the apex . • Murmur intensity and duration doesnot increase during inspiration. • The timing and quality of systolic and diastolic murmurs occasionally create the impression of a pericardial friction rub.
- 21. Arrythmias • On average, 35–50% of patients had arrhythmias at some time. • In some studies there was an association between arrhythmias and advancing age or increasing amount of tricuspid regurgitation. • Over half of the arrhythmias are supraventricular tachycardias of various types. • About one-quarter are paroxysmal or sustained atrialfibrillation or flutter. • A few are high-grade conduction defects. A minority are ventricular tachycardia, ventricular fibrillation.
- 22. INVESTIGATIONS
- 23. ECG • Tall wide P waves • RBBB – 72% to 92% • Severity is related to abnormal function of the SEPTAL leaflet • PR Prolongation – due to RA enlargement and long intra-atrial conduction times • Accesoory pathways – Ventricular preexcitation seen in 10-30%
- 25. CHEST XRAY • Severe Cardiomegaly • Cardiothoracic ratio > 0.6 • Was considered an indication for surgery
- 26. ECHOCARDIOGRAM • Gold Standard • Displacement Index >8 mm/m2
- 28. Celermajer index score/Great Ormond Street Echocardiography (GOSE) score
- 29. HIGH MORTALITY
- 30. Neonatal Ebstein • Neonatal Ebstein • Poor prognosis • Reported survival only 68% • Indiactions for surgery • Heart failure • Profound cyanosis
- 31. Initial management • Prostaglandin infusion • Initiation of mechanical Ventillation • Management of pulmonary Hypertension a) Nitric oxide b) Sildenafil • Diuretics for CHF
- 32. INDICATIONS FOR INTERVENTION • Cyanosis • Right sided failure • Poor functional capacity • Paradoxical emboli
- 33. INTERVENTIONAL OPTIONS • TV repair preferred to replacement • Repair fesibility – depends on ANTERIOR leaflet adequacy to form a monocusp /cone like structure
- 34. • 1970’s – Mayo Clinic – Danielson Monocusp Repair • 1988 – Fench – Carpentier Repair • 2004 – Ullman et al – Ventriculisation • 2007 – De Silva et al – Cone Reconstruction
- 35. TV Repair – CONE Reconstruction Dr Da Silva (Brazil)
- 36. PROGNOSIS • With satisfactory valve repair, medium and long term prognosis are good
- 37. THANK YOU
Editor's Notes
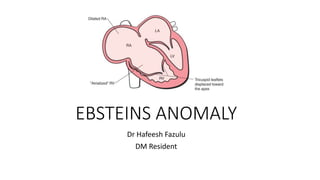
- The schematic demonstrates apical displacement (*) of the septal leaflet of the tricuspid valve and the displaced, long (sail-like) anterior leaflet. Note the large atrialized portion of the RV and dilated TVA.
- EC – endomyocardial layer
- • Brickner ME,et al N Engl J Med. 2000;342:334 –342. • Attenhoferet al. Mayo Clin Proc. 2005;80:361–368 . • Anderson et alCirculation. 1978;58(suppl):I-87–I-91.
- Calermejer
- The cone repair described by Dr. da Silva from Brazil when the anatomy allows, as this technique is the most anatomic of all the repair techniques described. Specially, some septal leaflet should be present, which facilitates this repair technique. The cone technique represents the most anatomic repair by completion of the delamination process of the TV, providing 360 degrees of leafet tissue around the AV junction with its hinge point at the AV groove (true annulus).