SEGMENTAL ANALYSIS OF CONGENITAL HEART DISEASE
•Download as PPT, PDF•
38 likes•7,225 views

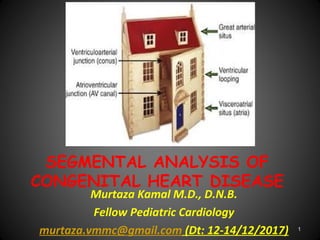
This document provides an overview of segmental analysis for congenital heart disease. It discusses the key segments that are analyzed which include thoraco-abdominal situs, pulmonary situs, atrial situs, ventricular situs and looping, connections between segments (venous, atrioventricular, ventriculoarterial), and abnormalities that can occur in each segment. The document emphasizes evaluating each segment in a systematic, sequential manner to identify abnormalities.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to SEGMENTAL ANALYSIS OF CONGENITAL HEART DISEASE
Similar to SEGMENTAL ANALYSIS OF CONGENITAL HEART DISEASE (20)
More from Dr. Murtaza Kamal MD,DNB,DrNB Ped Cardiology
More from Dr. Murtaza Kamal MD,DNB,DrNB Ped Cardiology (20)
Recently uploaded
Recently uploaded (20)
SEGMENTAL ANALYSIS OF CONGENITAL HEART DISEASE
- 1. SEGMENTAL ANALYSIS OF CONGENITAL HEART DISEASE Murtaza Kamal M.D., D.N.B. Fellow Pediatric Cardiology murtaza.vmmc@gmail.com (Dt: 12-14/12/2017) 1
- 2. MAUDE ELIZABETH SEYMOUR ABBOTT 1936 McGill University, Canada 1st systematic study Based on study of 1000 heart specimen 2
- 3. Richard Van praagh • 1964 • Pediatric Cardiologist • Boston Children Hospital, Massachusetts • Segmental approach to CHD 3
- 4. History Cont… • Kirklin(1973): Modified the segmental approach using concordance/discordance to describe connections between 3 main cardiac segments • Shinebourne/Anderson/Tynan(1976): Popularized the sequential segmental approach to CHD 4
- 5. 5
- 6. 6
- 7. THORACO-ABDOMINAL SITUS Situs: Topology/ spatial position of structureSitus: Topology/ spatial position of structure 1st segment evaluated is visceral situs Atrial and visceral situs considered together because they usually are concordant ( atrial and visceral situs are same) 7
- 8. Pulmonary Situs (Sidedness) • Determined by positions of morphologic rt & lt lungs • Pulmonary morphology, in turn, defined by relationship of PAs to their adjacent bronchi, and not by the number of lobes • PA of a morphologic right lung travels anterior to its upper and intermediate bronchi, whereas that of a morphologic left lung travels over its main bronchus and posterior to the upper lobe bronchus 8
- 9. Pulmonary Situs (Sidedness) Cont… • Rt bronchus branches, then RPA crosses it • LPA crosses lt bronchus, then it branches • Clinically, pulmonary situs may be inferred by comparing relative lengths of 2 main bronchi, as measured on a CXR that shows an air bronchogram • Distance from carina to origin of upper lobe bronchus is 1.5- 2.5 X greater for morphologic left lung than for right lung, and this ratio holds true regardless of the sidedness of the aortic arch 9
- 10. 10
- 11. The morphologically left bronchus is long, and it branches only after it has been crossed by its accompanying pulmonary artery, making the bronchus hyparterial. In contrast, the morphologically right bronchus is short, and is crossed by its pulmonary artery only after it has branched, giving an eparterial pattern of branching LR 11
- 14. 14
- 15. Cardiac malposition • Often an integral part of complex associated anomalies of visceral atrial situs • Prevalence 1 in 10, 000 live births Cardiac malpositions: Dextrocardia Mesocardia Levocardia (isolated) Ectopia cordis 15
- 17. 17
- 18. DEXTROCARDIA • Detro position • Dextro version • Mirror image dextrocardia 18
- 19. Dextroposition: Heart pushed/ pulled into right chest Push: Lt sided tension pneumothoax Lt congenital lobar emphysema Lt diaphragmatic hernia Pull: Hypoplasia/ agenesis of rt. lung DEXTROCARDIA 19
- 20. DEXTROCARDIA Cont… Dextroversion: Failure of pivoting of cardiac apex to left, frequently associated with A-V discordance Mirror-image dextrocardia with atrial situs inversus There may be major and complex pathology associated with this type of dextrocardia 20
- 21. 21
- 22. MESOCARDIA Location of heart with cardiac base apex axis directed to midline of thorax or with ventricular apices equally directed to both right and left sides This is often ignored as being infrequent and atypical 22
- 23. Isolated levocardia Occurring in conjunction with situs inverses and situs ambiguous An abnormal atrial and visceral situs, the heart is in its normal location in the left hemi thorax with the apex pointing to left 23
- 24. Ectopia Cordis • Partially/ completely exteriorized • Pentalogy of Cantrell: – 1. Deficiency of ant. Diaphragm – 2. Midline supra umbilical abdominal wall defect – 3. Defect in diaphragmatic pericardium – 4. CHD – 5. Defect of lower sternum 24
- 25. BASIC CARDIAC POSITIONS 95% CHD 100% CHD 3-5%CHD<1%CHD 25
- 26. 26
- 28. SEGMENT CONNECTION Great veins Atria Ventricles Great arteries Venoatrial Atrioventricular Ventriculoarterial 28
- 29. 29
- 30. 30
- 31. VENOUS SEGMENT Systemic veins: IVC, hepatic veins, SVC, CS Pulmonary veins HEPATIC VEINS: SC view, drains into RA CS – RA IVC – RA 31
- 32. Venous Segment Cont… ABNORMALITY OF IVC: Subcostal view Interrupted IVC (Polysplenia): Large azygous vein entering SVC seen along the spine in abdomen, can be either right or left sided Even then there is another vein draining into RA called: Suprahepatic IVC Suprahepatic IVC always drains into RA Suprahepatic IVC differentiated from IVC in being small and can’t be traced below liver 32
- 33. SVC • SVC: Single right sided • Subcostal view, high parasternal or suprasternal view • LSVC: • Connected to CS posteriorly/ laterally • Border of LA (dilated CS) • Directly visualized in a long axis plane • Parasternal short axis images: Circular vessel anterior to LPA near bifurcation • SVC less reliable than IVC for situs 33
- 34. CS & LSVC 34
- 35. Pulmonary veins • Subcostal, suprasternal, apical • Color Doppler: Distinguishes from atrial appendage • 4 in number • Left 2 veins may join: 3 entries into LA 35
- 36. ATRIAL SITUS The identification of the morphologic right atrium is important for establishing atrial situs Anatomic hallmark is the limbus of the fossa ovalis 36
- 37. Atrial Situs • Describes location of atria • Solitus: Morphological RA on rt • Inverses: Morphological RA on lt • Ambiguous: Undifferentiated atria 37
- 38. Right atrium Left atrium SEPTUM: Limbus of fossa ovalis Flap valve of fossa ovalis APPENDAGES: Broad based, triangular, anterior Long and narrow, finger like, posterior MYOCARDIAL FEATURES: Crista terminalis, tinea sagittalis, extension of pectinate muscles towards AV valve Pectinate muscle confined to appendage VEINS: Receives IVC, suprahepatic IVC, SVC, coronary sinus Receives pulmonary veins 38
- 40. 40
- 41. Subcostal sagittal views demonstrating eustachian valve (arrow in A) and flap valve (arrow in B). 41
- 43. 43
- 44. Viscero atrial situs and its abnormality Isomerism of Lt atrial appendage: •B/l lt atrial appendage: Smooth pectinate muscles •Interrupted IVC: 85% Isomerism of Rt atrial appendage: • B/l rt atrial appendage: Coarse pectinate muscles •Abscent coronary sinus: 100% •Abnormal relation of aorta and IVC 44
- 46. 46
- 47. VENTRICULAR SITUS AND MORPHOLOGY Right ventricle Left ventricle Large apical trabeculations Small apical trabeculations Coarse septal surface Smooth upper surface Moderator band No moderator band Receives tricuspid valve Receives mitral valve Tricuspid-pulmonary discontinuity Mitral-aortic continuity Crescentic in cross section Circular in cross section Thin free wall (3-5 mm) Thick free wall (12-15 mm) 47
- 48. Apical four-chamber view in a patient with ventricular inversion with L-TGA 48
- 49. VENTRICULAR LOOPING After morphology Determine looping Bulboventricular loop: Describes location of ventricles d-Loop: Morphologic RV on right l-Loop: Morphologic RV on left 49
- 50. VENTRICULAR LOOPING Cont… Performed by imagining one is standing on the right ventricle side facing the right ventricular face of the interventricular septum The palm of one hand is placed against the septum The looping is determined by establishing which of the two hands allow the thumb to point into the atrioventricular valve and the fingers to point into the outflow tract If rt. hand meets criteria: d-looped, if lt hand meets criteria: l-looped 50
- 51. The palmar surface of the right hand can be placed on the septal surface of the normal morphologically right ventricle with the thumb in the inlet component and the fingers extending into the ventricular outlet. (d-ventricular loop.) 51
- 52. The mirror-imaged normal heart. In this setting, it is the palmar surface of the left hand that can be placed on the septal surface of the morphologically right ventricle with the thumb in the inlet and the fingers in the outlet. (l-ventricular loop) 52
- 53. VENTRICULAR LOOPING Cont… In general, convexity of aorta points to the position of the right ventricle and thus helps indicate bulboventricular loop Definitive indicator of bulboventricular loop, however, is relative positioning of ventricular inlets/ AV valves Thus, in a d-loop the tricuspid valve is to the right of the mitral valve, and in an l-loop the tricuspid valve is to the left of the mitral valve In a normal d-loop the apex pivots to the left hemithorax; in a "normal" l-loop (i.e., one in the setting of situs inversus) the apex pivots to the right hemithorax 53
- 54. SINGLE VENTRICLE • Single ventricle: Determined by morphology of ventricle • Single vent of RV morphology: Hypo plastic LV remnant, posterior to main ventricular chamber • LV morphology: Rudimentary RV, anterior 54
- 55. 55
- 56. 56
- 57. AV Connections and AV Valve Morphology First see: Bi/uni ventricular connection If double see: AV concordance/discordance If single ventricle see: Double inlet, single inlet, common inlet 57
- 58. 50% rule Anderson et al: Rule of 50% for determining whether a cardiac chamber is a ventricle For the assessment of AV connections, an atrium is considered to join the ventricle into which >50% of the valve orifice empties This rule states that a chamber is a ventricle if it receives 50% more of an inlet The inlet consists of the fibrous ring of the AV valve and need not always include a patent AV valve with well formed valve leaflets 58
- 59. 50% RULE Cont… Eg: In HLHS with aortic and mitral atresia, the fibrous ring of the MV contains an imperforate membrane and is situated over the small LV Thus, this small left sided chamber is a ventricle because it receives 100% of an inlet A chamber need not have an outlet to be a ventricle The rule of 50% has also been used to define VA connections Thus, if 50% or more of a great artery arises above a chamber, the great artery is defined as being 59
- 60. 50% RULE IN AV, VA • A great vessel should be related to a ventricle by 50% of its dimension to be considered committed to it • Av valve is committed to that ventricle to which >50% of that valve is connected 60
- 62. ATRIOVENTRICULAR VALVE MORPHOLOGY Tricuspid valve Mitral valve Septal chordal attachments No septal chordal attachments Low septal annular attachment High septal annular attachment Triangular orifice (midleaflet) Elliptical orifice (midleaflet) Three leaflets Two leaflets Several papillary muscles Two large papillary muscles Empties into right ventricle Empties into left ventricle 62
- 64. OVERRIDING AV VALVE Abnormality of AV valve alignment or connection in which one valve annulus opens into another chamber through a VSD 64
- 65. STRADDLING A feature of the tensor apparatus (chordae tendineae and papillary muscles) of an AV valve and indicates anomalous insertion into the contralateral ventricle, either along its septum or its free wall 65
- 66. 66
- 67. 67
- 68. VENTRICULOARTERIAL CONNECTION If Ao from LV and PA from RV: Concordant If Ao from RV and PA from LV: Discordant Origins of Ao and PA are evident on PLAX view, sweeping the transducer inferiorly from the basal short-axis view, A5CV and SC coronal and sagittal views 3rd type of VA connection: Double outlet, almost always from RV Final type of VA connection: Single outlet (truncus arteriosus) 68
- 69. VA Connection Aorta: •Coronary artery •Carotids •Absence of proximal division PA: •Bifurcation 69
- 70. Parasternal short-axis images demonstrating different relationships between the great vessels. An echocardiogram from an infant with tetralogy of Fallot and pulmonary atresia demonstrates the identifying features of a pulmonary artery (MPA) with its bifurcation into right and left pulmonary arteries (RPA, LPA). The great vessels are normally related 70
- 71. 71
- 72. 72
- 73. CONAL MORPHOLOGY Conus/ infundibulum: Cavitary space formed by muscular segment of heart that connects ventricles with great arteries and separates the AV and semilunar valves Abnormalities in conal development consist of variations in the presence, length and diameters of subpulmonary and subaortic conus These variations can lead to (or be associated with) complex malformations, such as TOF, IAA,TGA and DORV 73
- 74. Subpulmonary conus - Best identified in subcostal views In normal heart: Conus- Nearly vertical tubular outflow portion of RV Separated from nearly horizontal right ventricular inflow portion by distinct muscle bands These muscle bands form a near- circular rim formed by parietal band anteriorly, crista supraventricularis posteriorly, and septal band medially and prohibit PV to AV valve continuity 74
- 75. Conus Cont… Subaortic conus is evident on subcostal coronal and sagittal views Persistence of subaortic conus and involution of subpulmonic conus is the usual conal relationship in d- (or l-) TGA Persistence of subaortic conus prohibits continuity of the aortic valve to either AV valve, and involution of subpulmonary conus allows continuity between PV and both AV valves in TGA 75
- 76. BILATERAL CONUS B/l persistence of the subarterial conus usually results in DORV Because the main goal of surgical correction of DORV is to connect the aorta with the morphologic left ventricle through VSD, it is important to determine the conal relationships with each other and with the great vessels 76
- 77. BILATERAL CONUS When 2 coni are present, their relationship may be classified as either anterior/posterior or side-by-side With the anterior/posterior conal relationship, the ventricular septal defect is usually subaortic; with the side-by-side relationship, the defect is usually subpulmonic The conal relationship can be determined by subcostal coronal and sagittal imaging with anterior/posterior and left/right sweeping, respectively 77
- 78. ABSENT CONUS A rare type of d-transposition can exist in the context of bilaterally deficient subarterial conus This results in an unusual heart in which d-TGA exists with a doubly committed VSD and a posterior aorta Associated with DOLV 78
- 79. 79
- 81. Great Artery Relations 8 basic types of great artery relationships are possible based on the aortic and pulmonary valve positions at the level of the semilunar valves • Right posterior aorta (normally related) Right lateral aorta (side by side) Right anterior aorta (d-malposed) Directly anterior aorta Left anterior aorta (l-malposed) Left lateral aorta (left side by side) Left posterior aorta (inverted normal) Directly posterior aorta. 81
- 82. 82
- 83. 83
- 84. ARCH OF AORTA Unexpected position of aortic arch: Well recognized associated anomaly of conditions such eg. TOF/ Truncus Distinction should be made b/w position of arch and side of descending aorta, particularly in describing vascular rings Side of aortic arch depends on whether it passes to right or left of the trachea Position of descending aorta is defined relative to vertebral column 84
- 85. ARCH OF AORTA Cont… Aorta lies more posterior in center of Visualized in PLAX,PSAX, A5CV,SC , and suprasternal notch views Arch best seen in subcostal oblique view and suprasternal views Side of arch diagnosed by sweeping transducer in suprasternal long-axis view and noting the relationship of the arch to the trachea, the rings of which resemble a stack of coins 85
- 86. This transducer position allows visualization of the ascending aorta (Asc), aortic arch (Arch), origin of the brachiocephalic vessels (arrows), descending thoracic aorta (Dsc), and right pulmonary artery (*). ARCH OF AORTA LONG-AXIS 86
- 87. The short-axis view of the aortic arch is obtained by rotating the transducer clockwise, which also allows visualization of the right pulmonary artery (RPA) in its long-axis format, located inferiorly to the aortic arch (Arch). Inferior to RPA is the left atrial (LA) cavity with connections of the four pulmonary veins (arrows SHORT-AXIS VIEW 87
- 88. 88
- 89. FINAL DIAGNOSIS • SS, LEVOCARDIA, NORMAL SYSTEMIC & PULMONARY VENOUS COMMUNICATIONS, NRGAs, AV & VA CONCORDANCE, INTACT IA & IV SEPTUM, NO PDA, GOOD SIZED CONFLUENT BPAs, NORMAL ARCH, NO COA, NORMAL CORONARIES, NORMAL SIZED CHAMBERS, GOOD BV FUNCTION, NO VEGETATION/ CLOT OR PE 89
- 90. THANKS FOR UR PATIENCE 90