Download to read offline
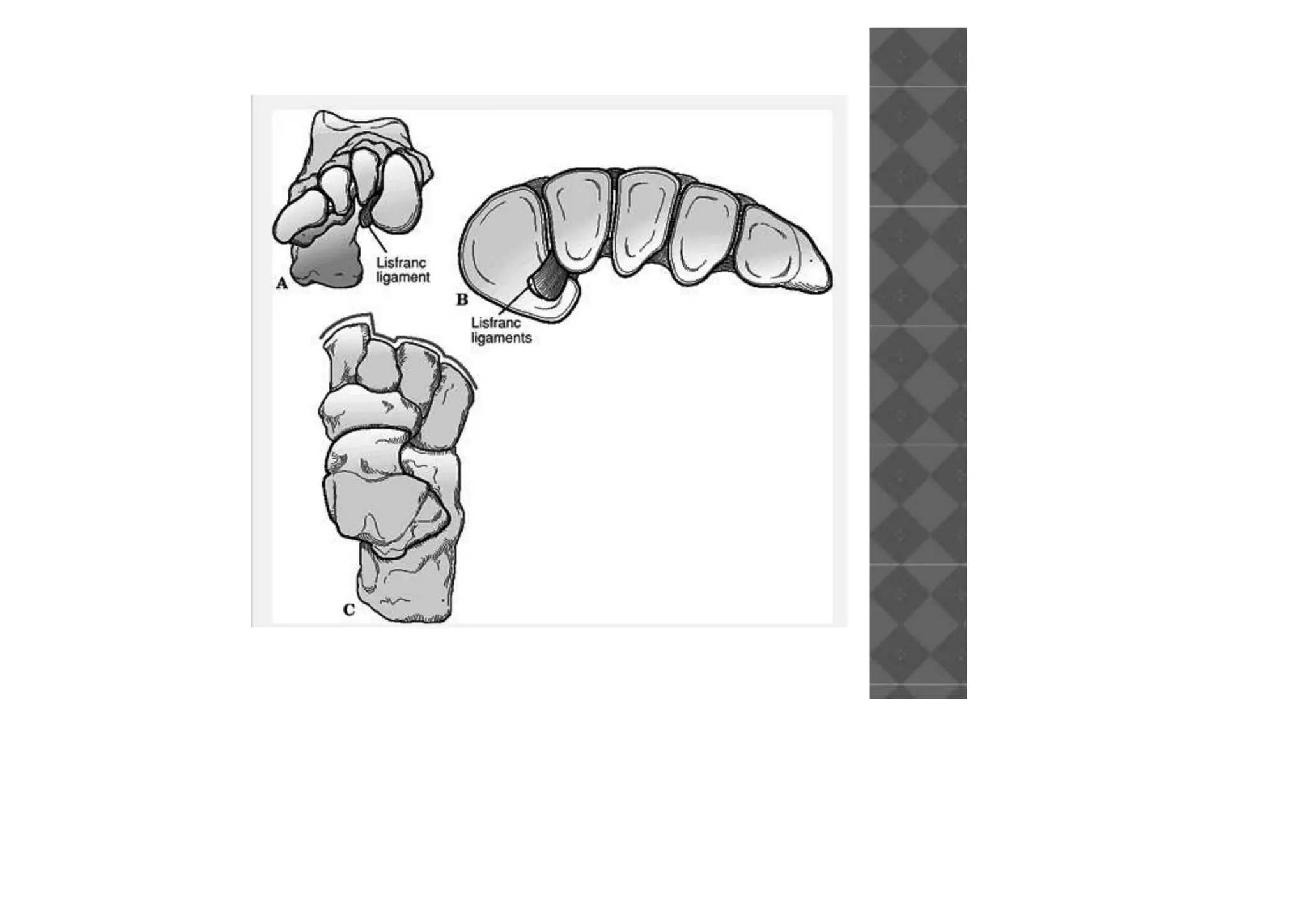
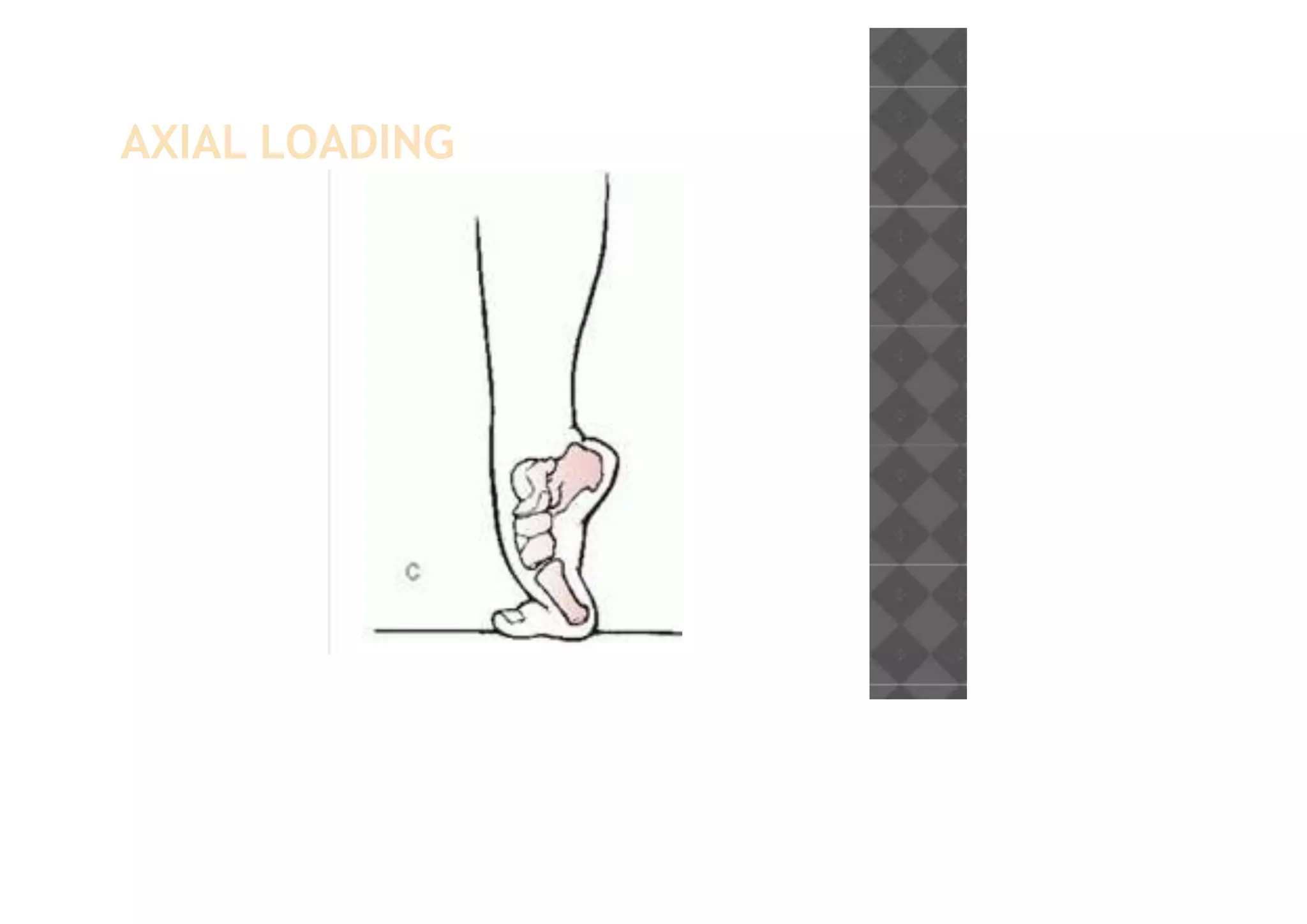
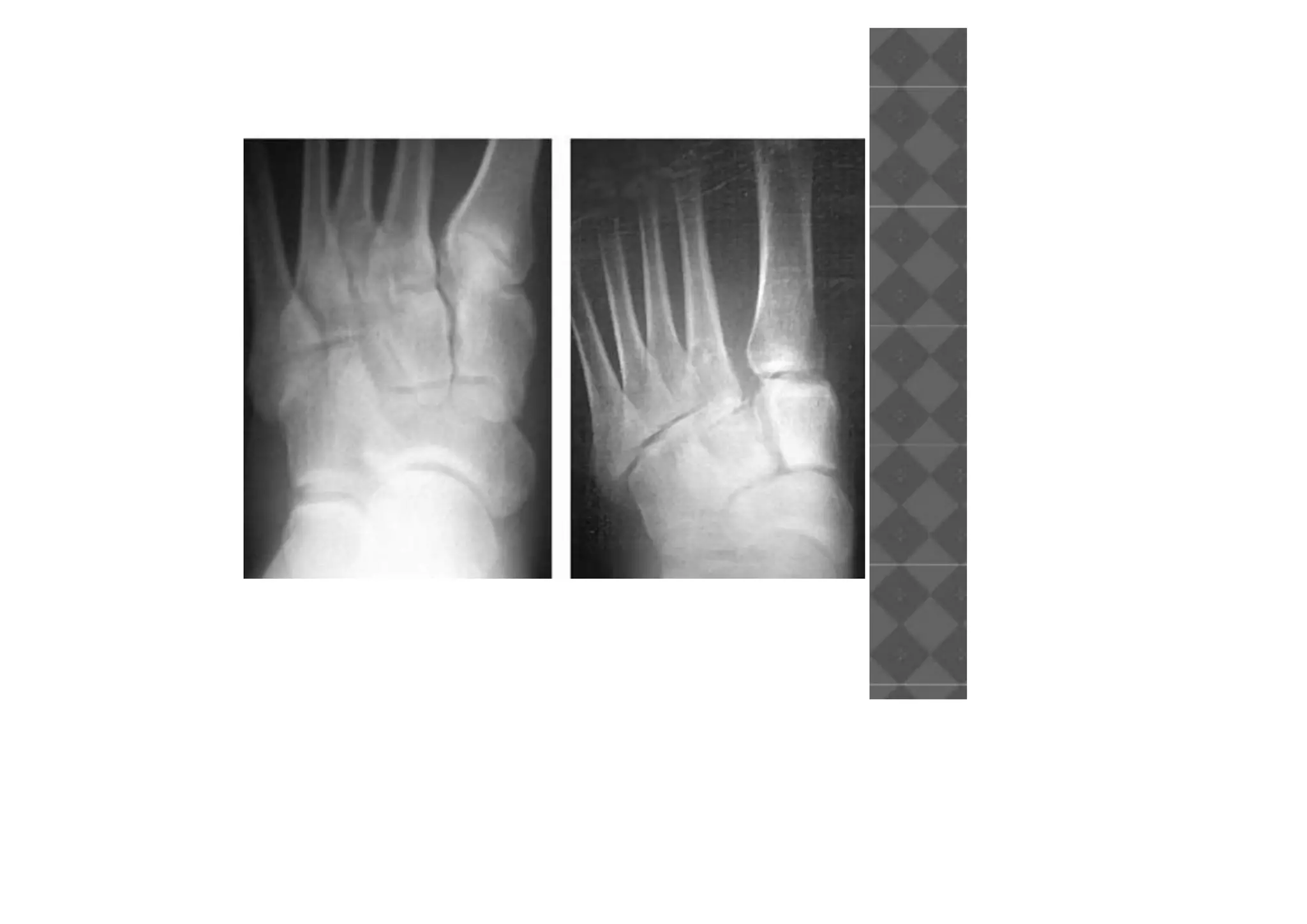
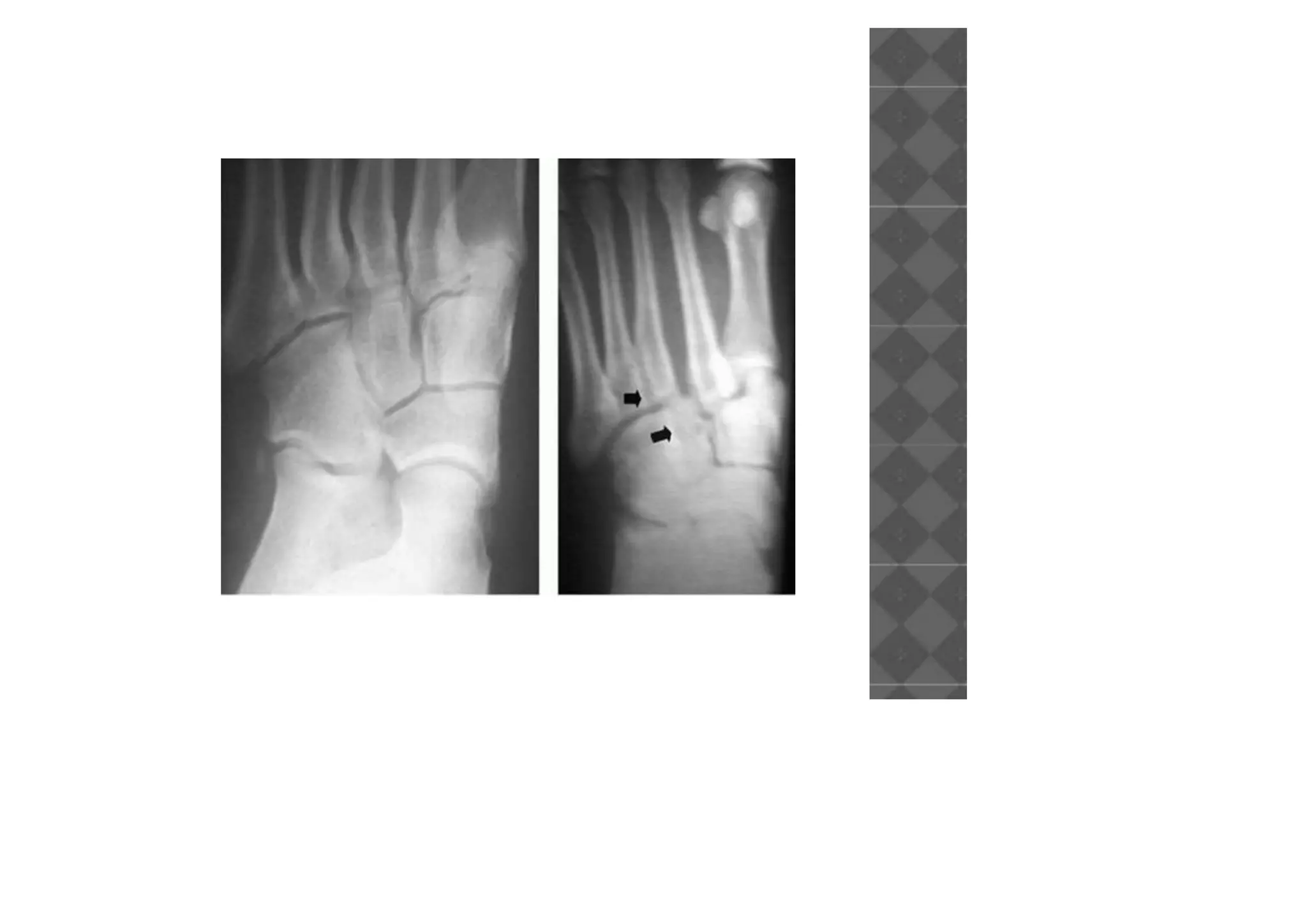
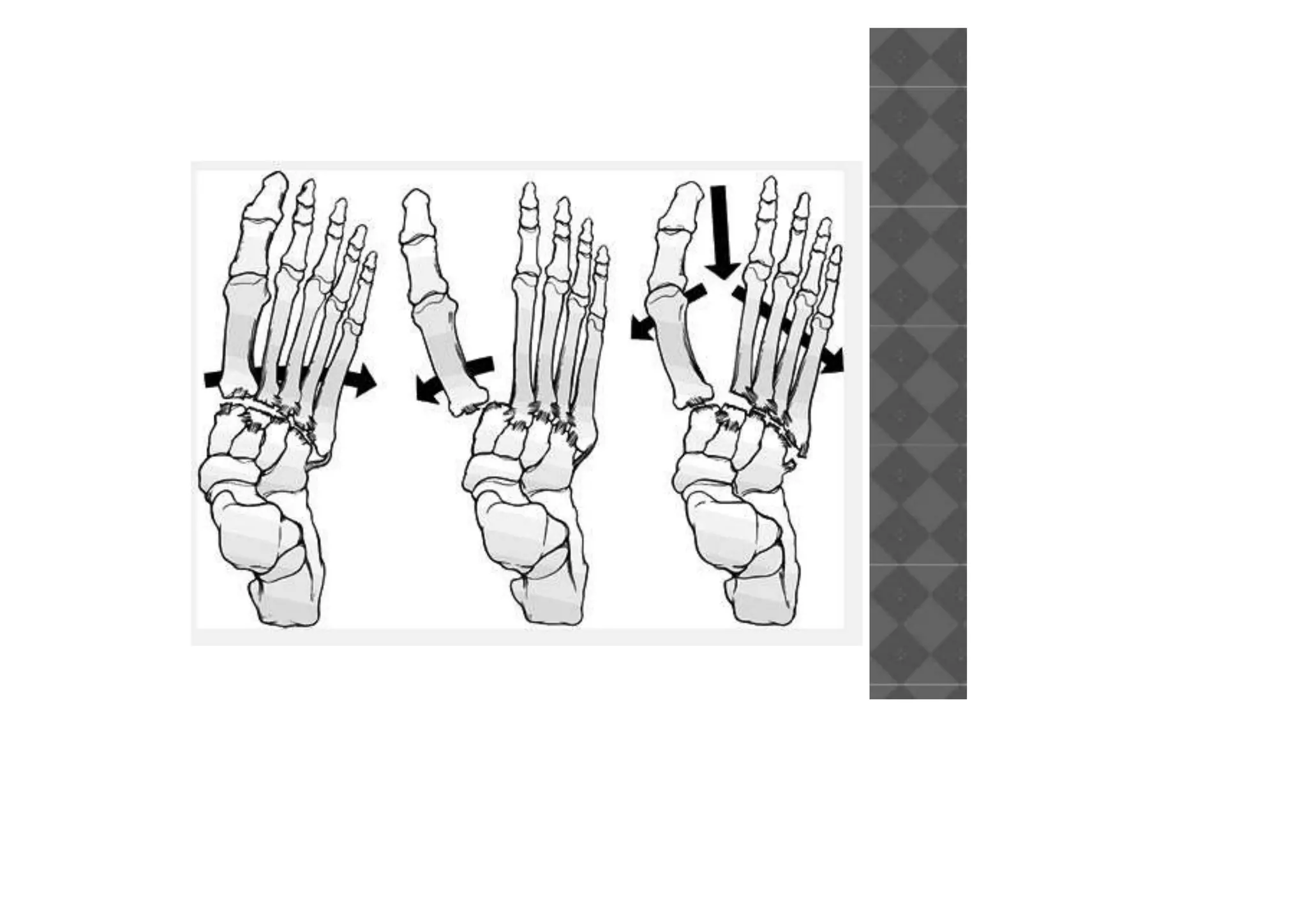
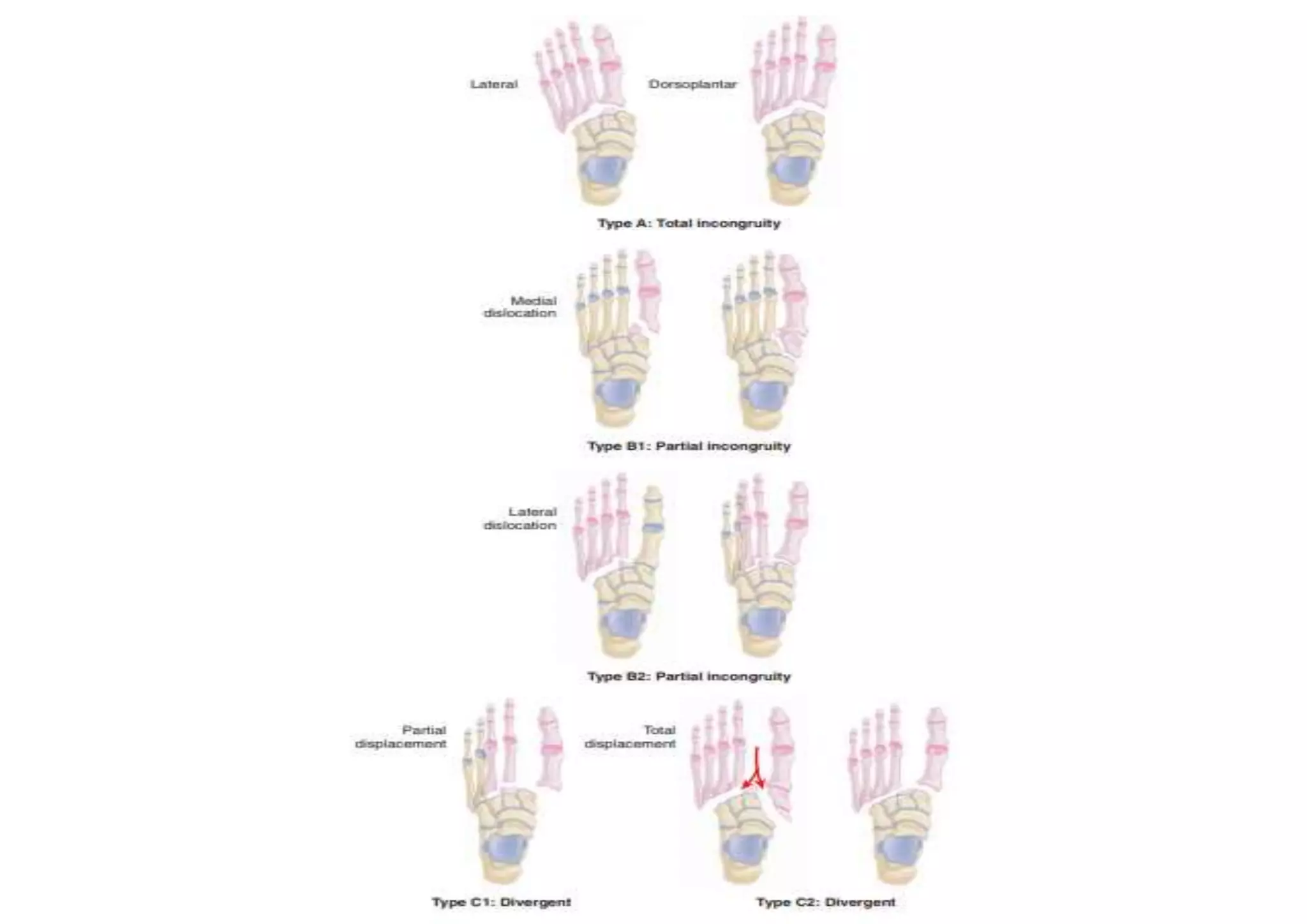

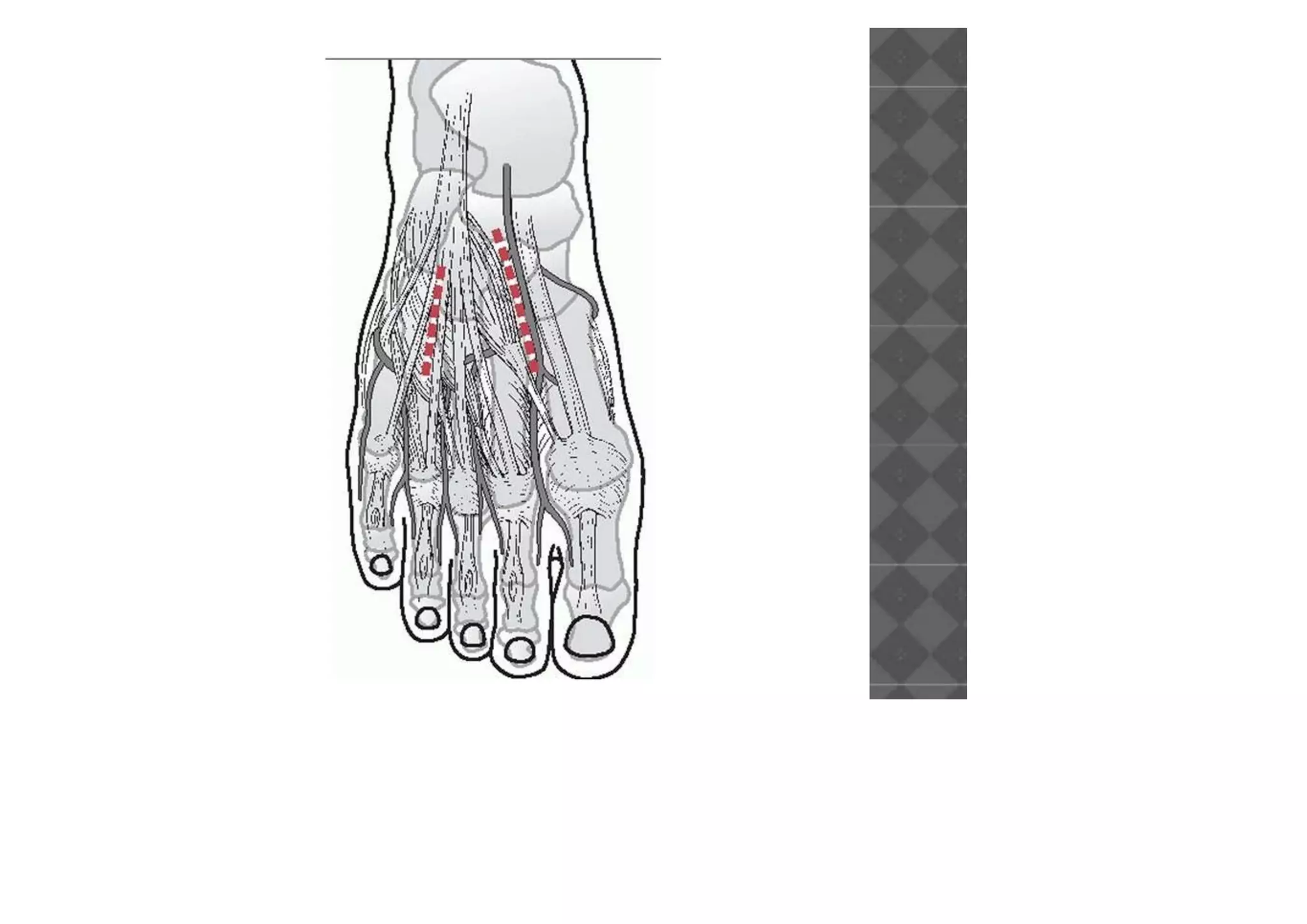


This document discusses Lisfranc injuries, which involve fracture or ligament disruption of the tarsometatarsal joint complex. It describes the anatomy of the Lisfranc joint and surrounding ligaments. Common mechanisms of injury are twisting of the forefoot or axial loading of a fixed foot. Clinical evaluation looks for foot deformity, swelling, and tenderness. Radiographs are used to diagnose and classify the injury based on displacement patterns. Treatment options include casting for nondisplaced injuries or open reduction and internal fixation for displaced fractures. Complications can include arthritis, stiffness, and neurovascular problems.























































































