Downloaded 67 times

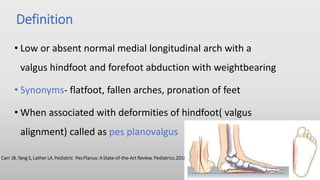
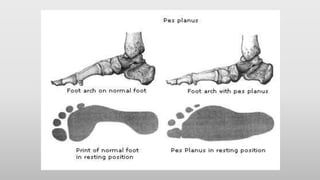
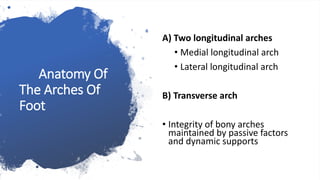

























Planovalgus foot, also known as flatfoot, is characterized by a low or absent medial longitudinal arch and hindfoot valgus. The document discusses the anatomy and development of the foot arches, causes of pediatric and adult flatfoot including posterior tibial tendon dysfunction, and treatment options ranging from orthotics to surgery. Surgical procedures discussed include calcaneal osteotomies, tendon lengthening/transfer, and arthrodesis. Complications and special flatfoot conditions like tarsal coalition and congenital vertical talus are also summarized.































![flat foot.ppt [pes planus ] #physio.# rehabilitation](https://cdn.slidesharecdn.com/ss_thumbnails/flatfoot-240310065759-517e9bef-thumbnail.jpg?width=640&height=640&fit=bounds)



































