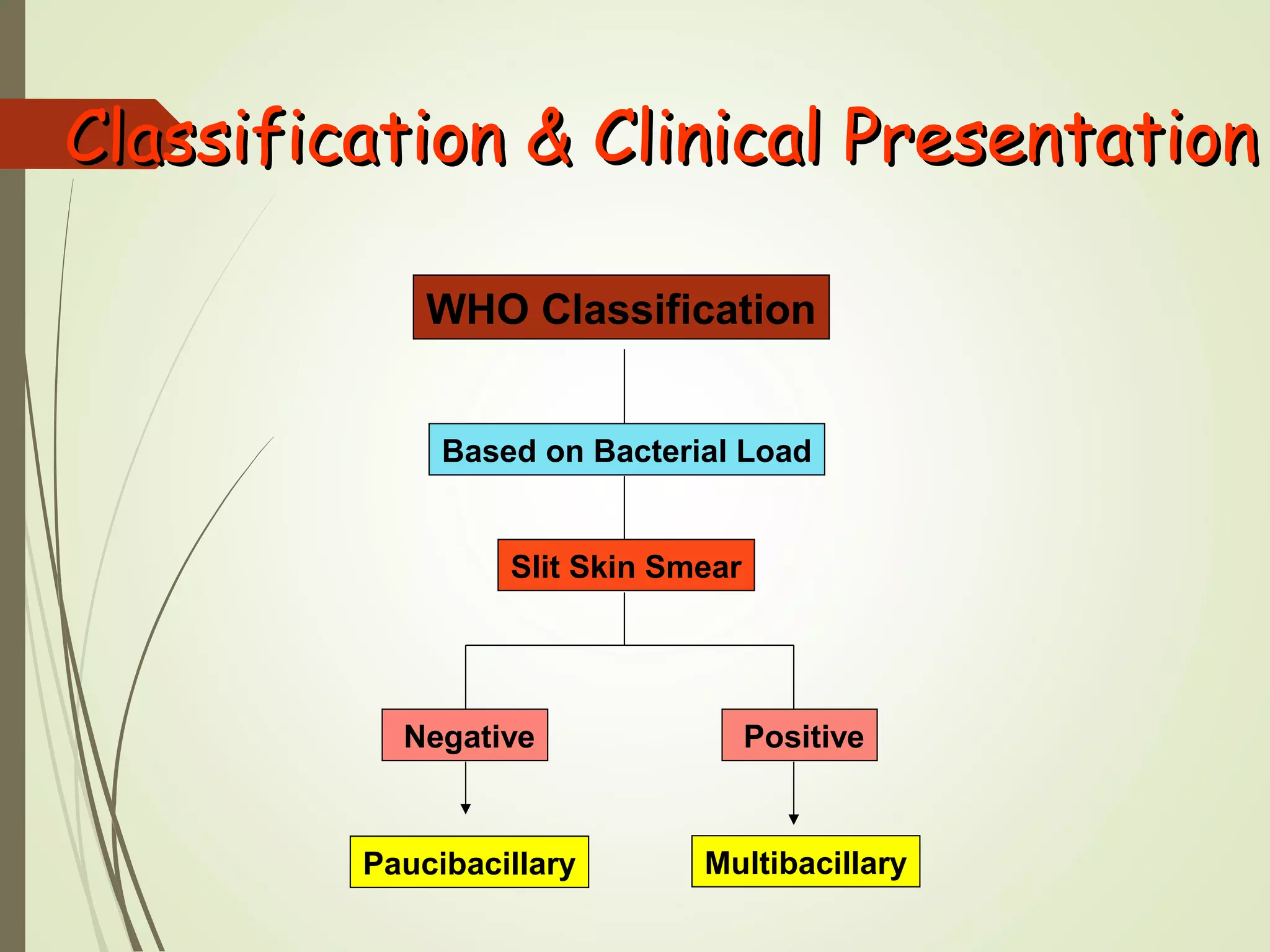
Leprosy, also known as Hansen's disease, is a chronic infectious disease caused by Mycobacterium leprae. It primarily affects the skin and peripheral nerves. Leprosy remains a public health problem in many tropical and subtropical countries. It is classified based on clinical, bacteriological, immunological and histopathological features. Complications can include reactions, peripheral nerve damage leading to numbness and deformities, and eye and bone complications. Treatment involves multidrug therapy to cure the disease and prevent further disability.