Downloaded 733 times



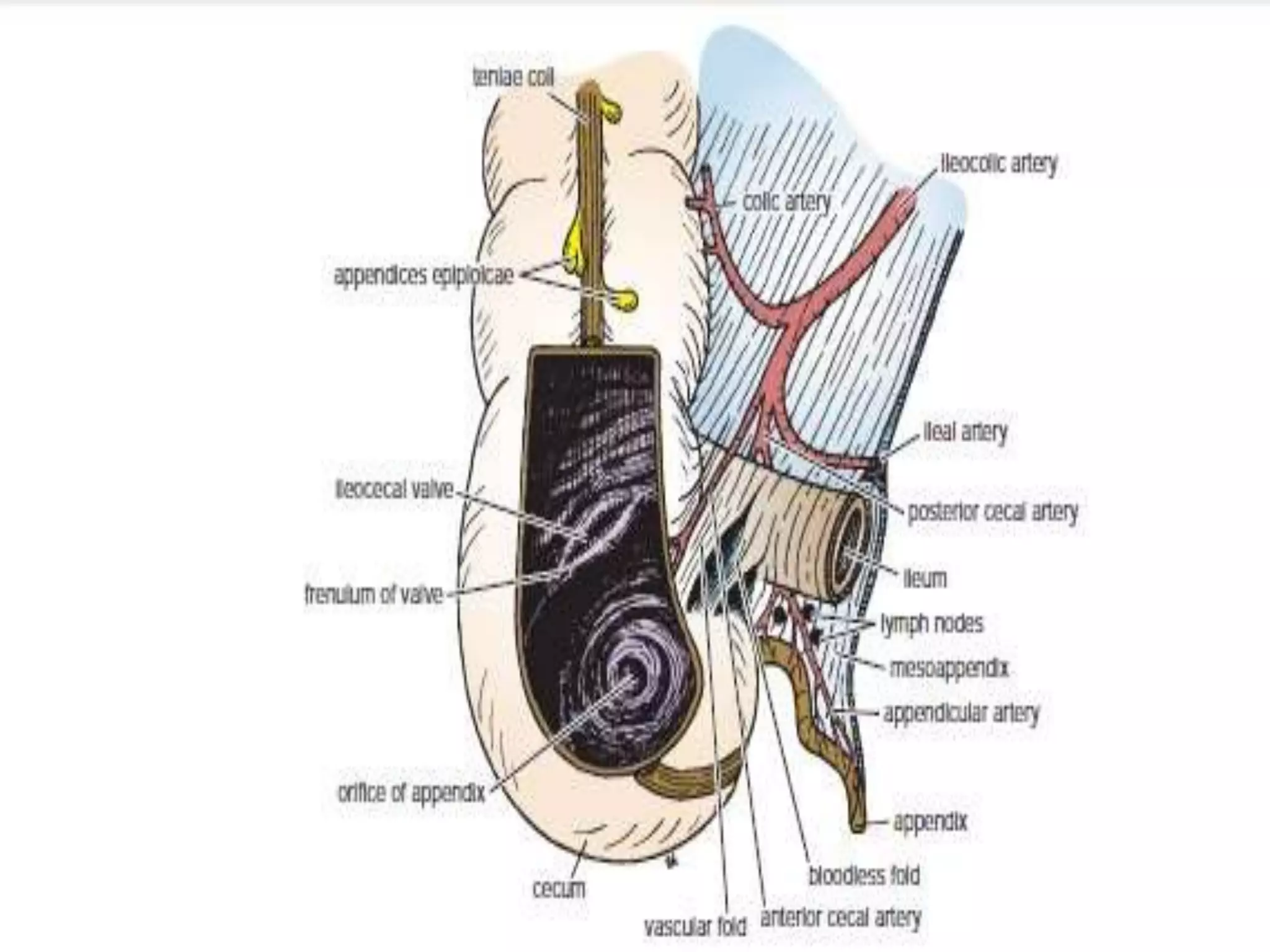




















The document provides a comprehensive overview of the anatomy and functions of the large intestine, detailing its sections: cecum, appendix, ascending colon, transverse colon, descending colon, sigmoid colon, rectum, and anal canal. Each section is described in terms of location, structure, blood supply, nerve supply, and relationships with surrounding organs. Additionally, it discusses the ileocecal valve and various anatomical features relevant to each section of the large intestine.























































































