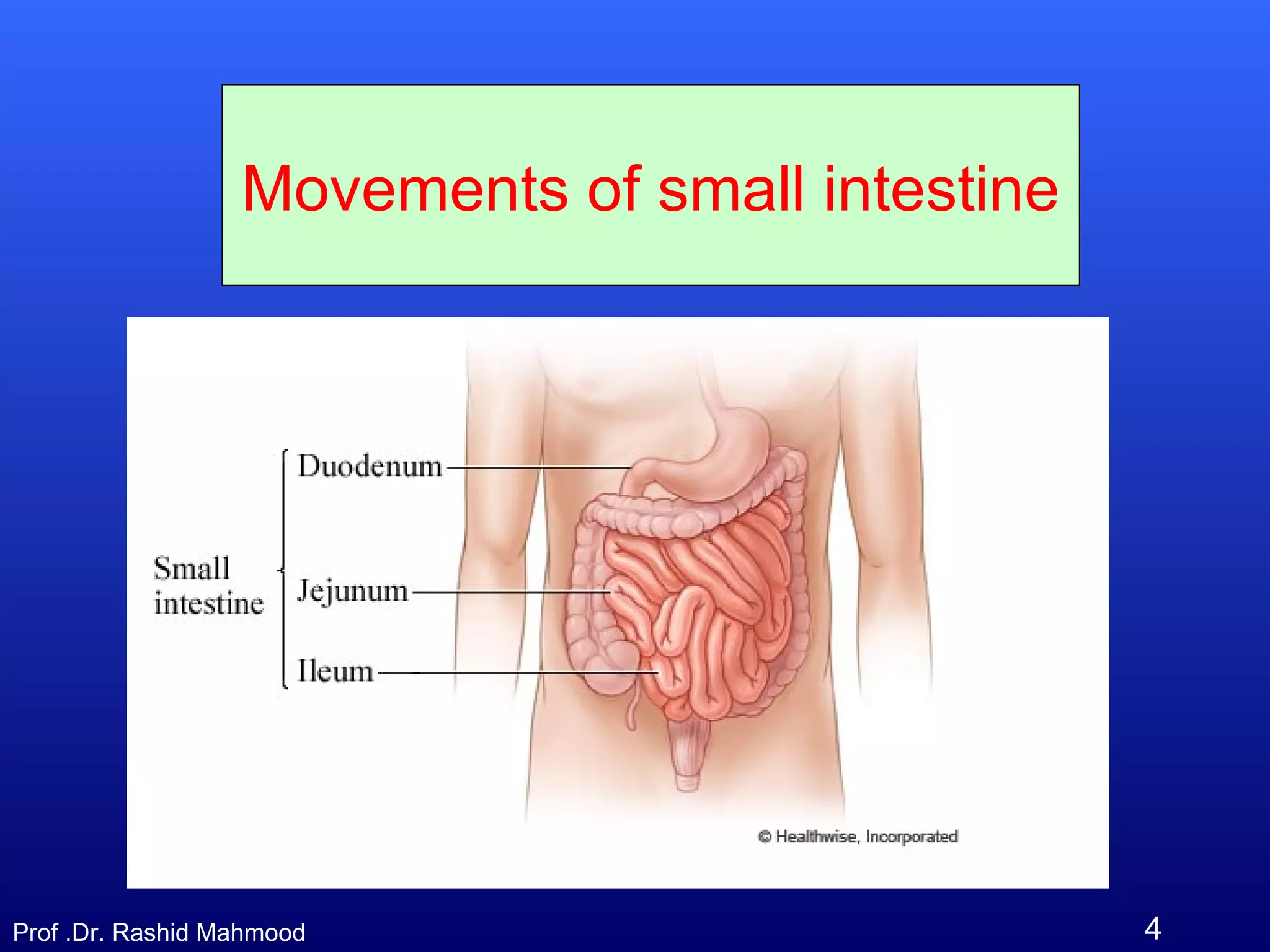
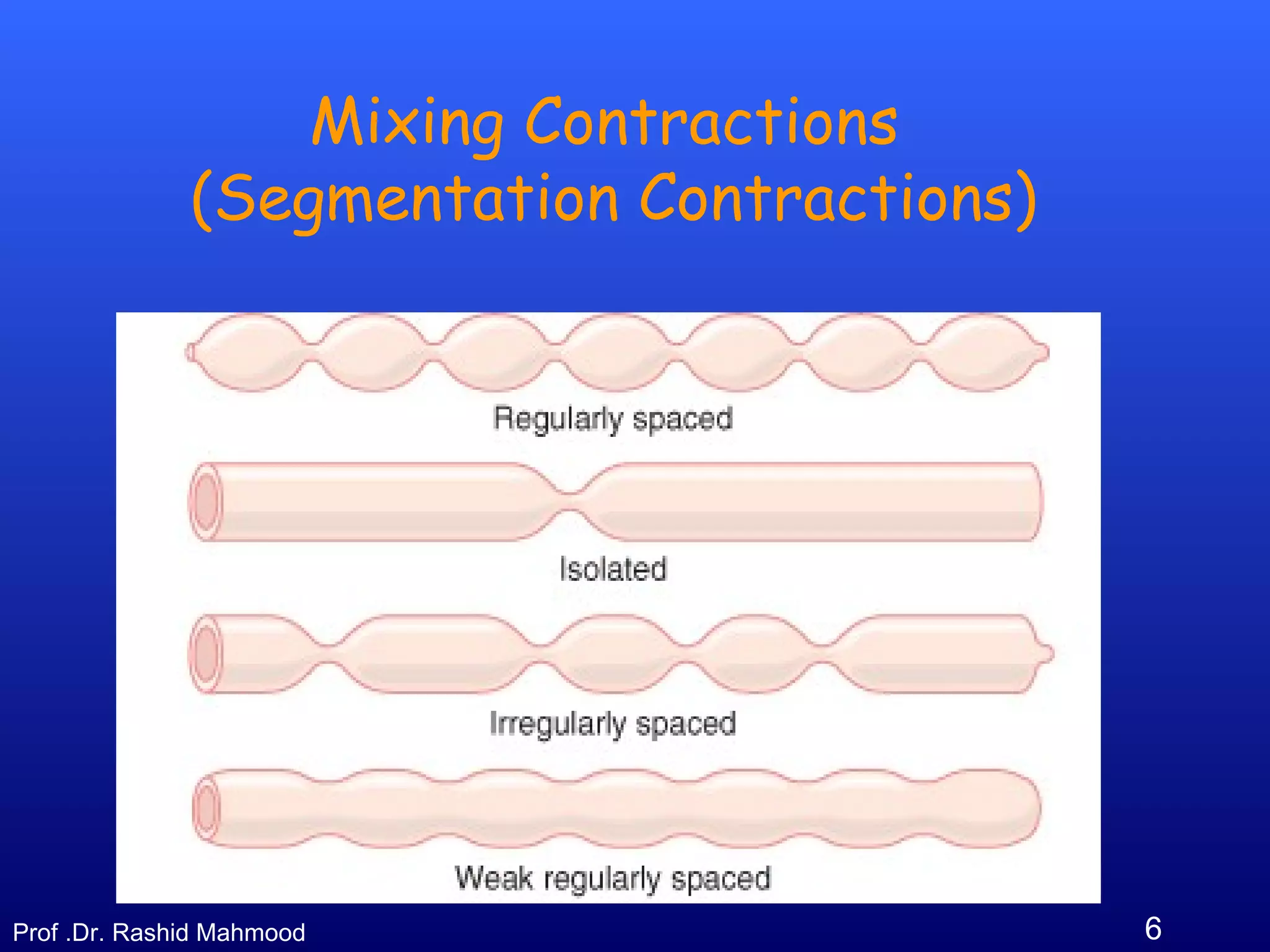
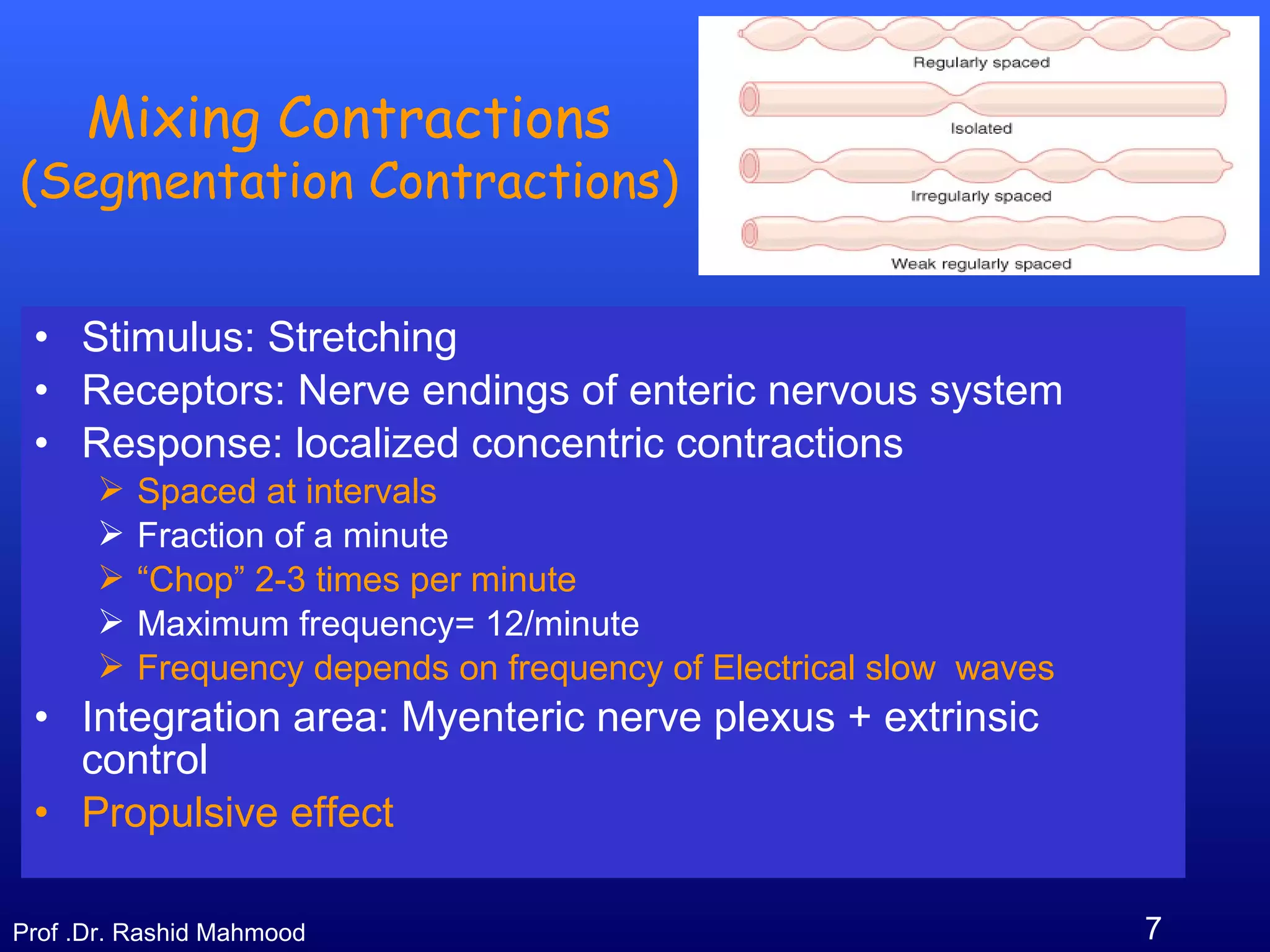
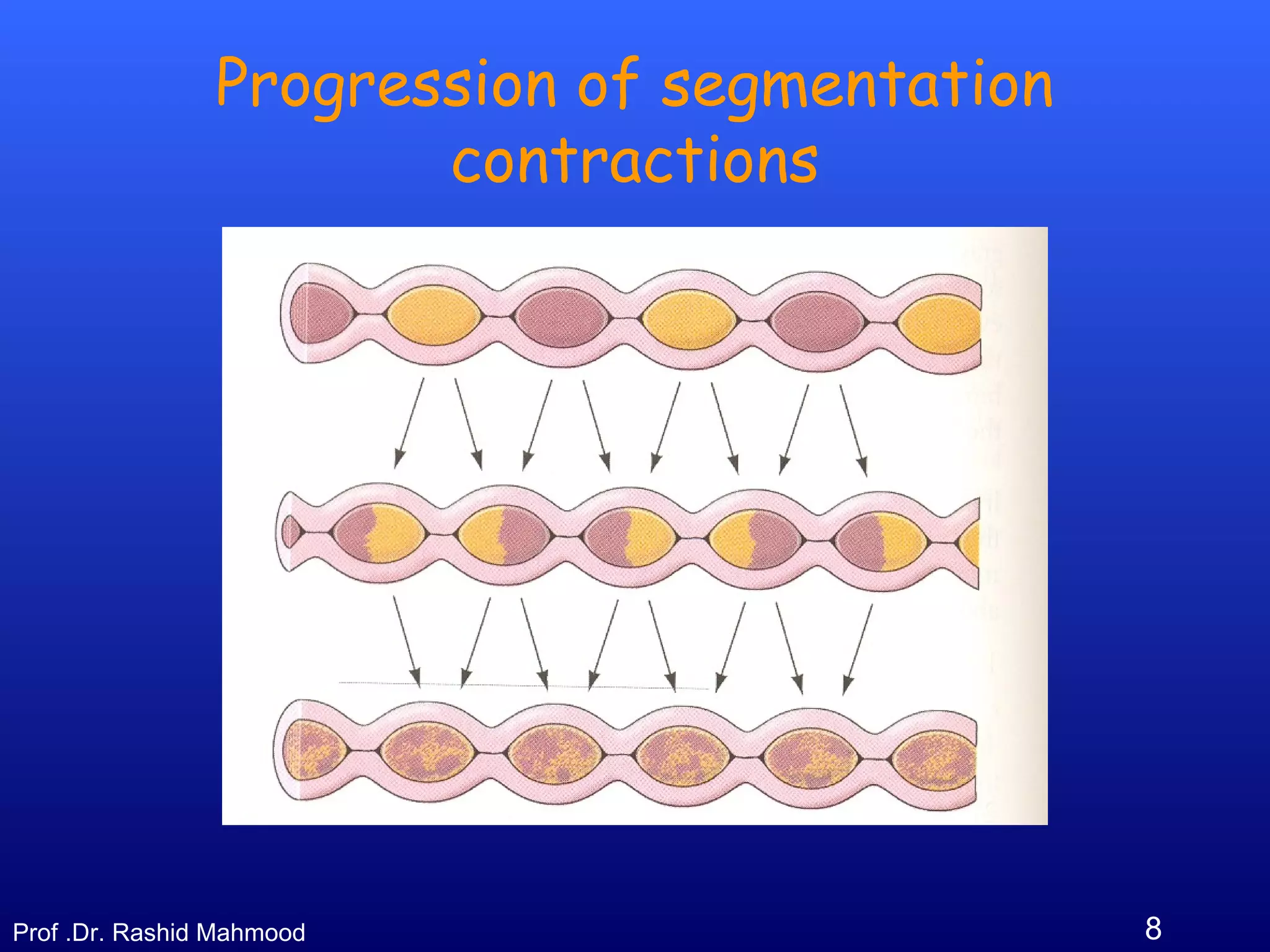
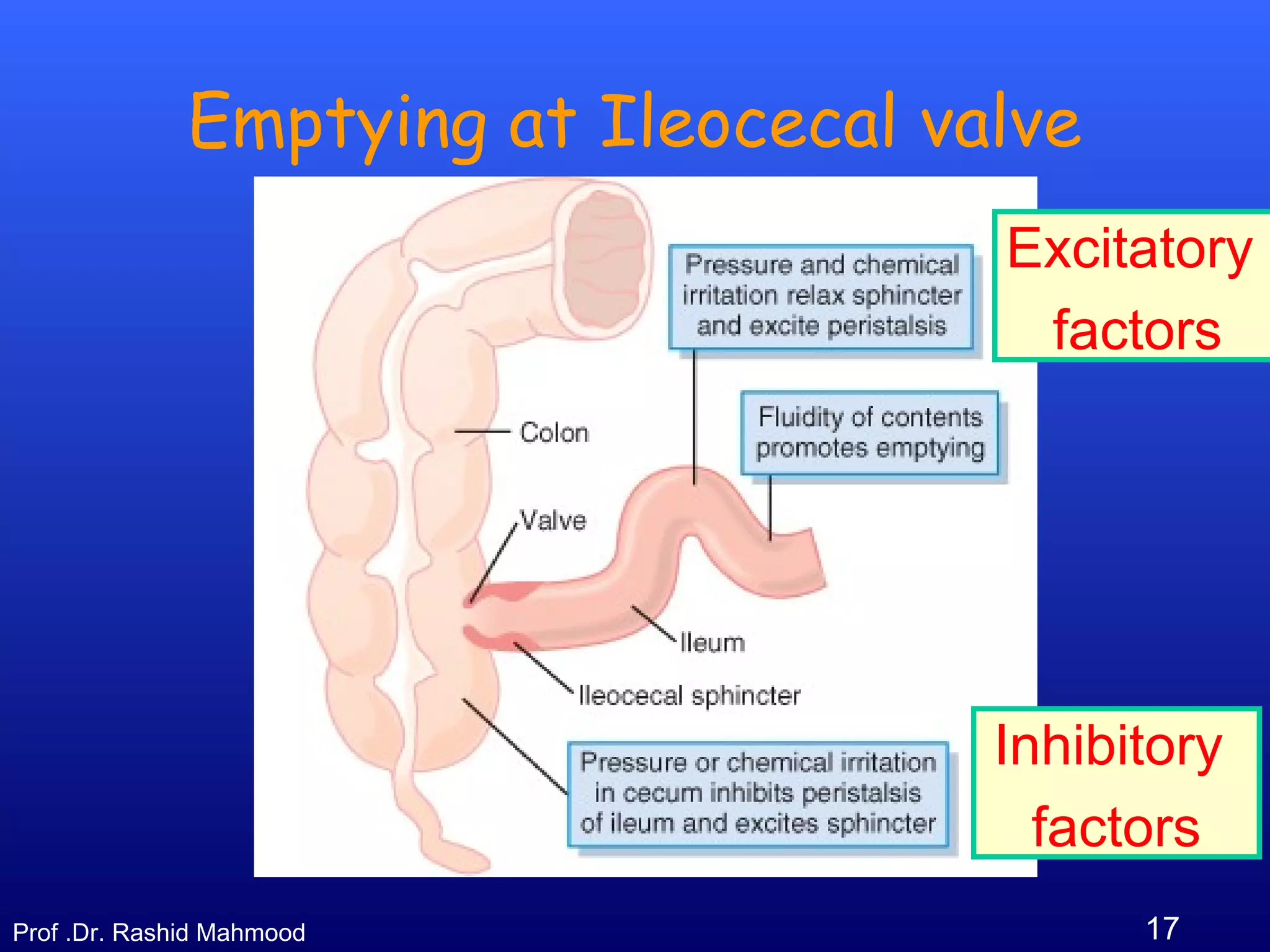
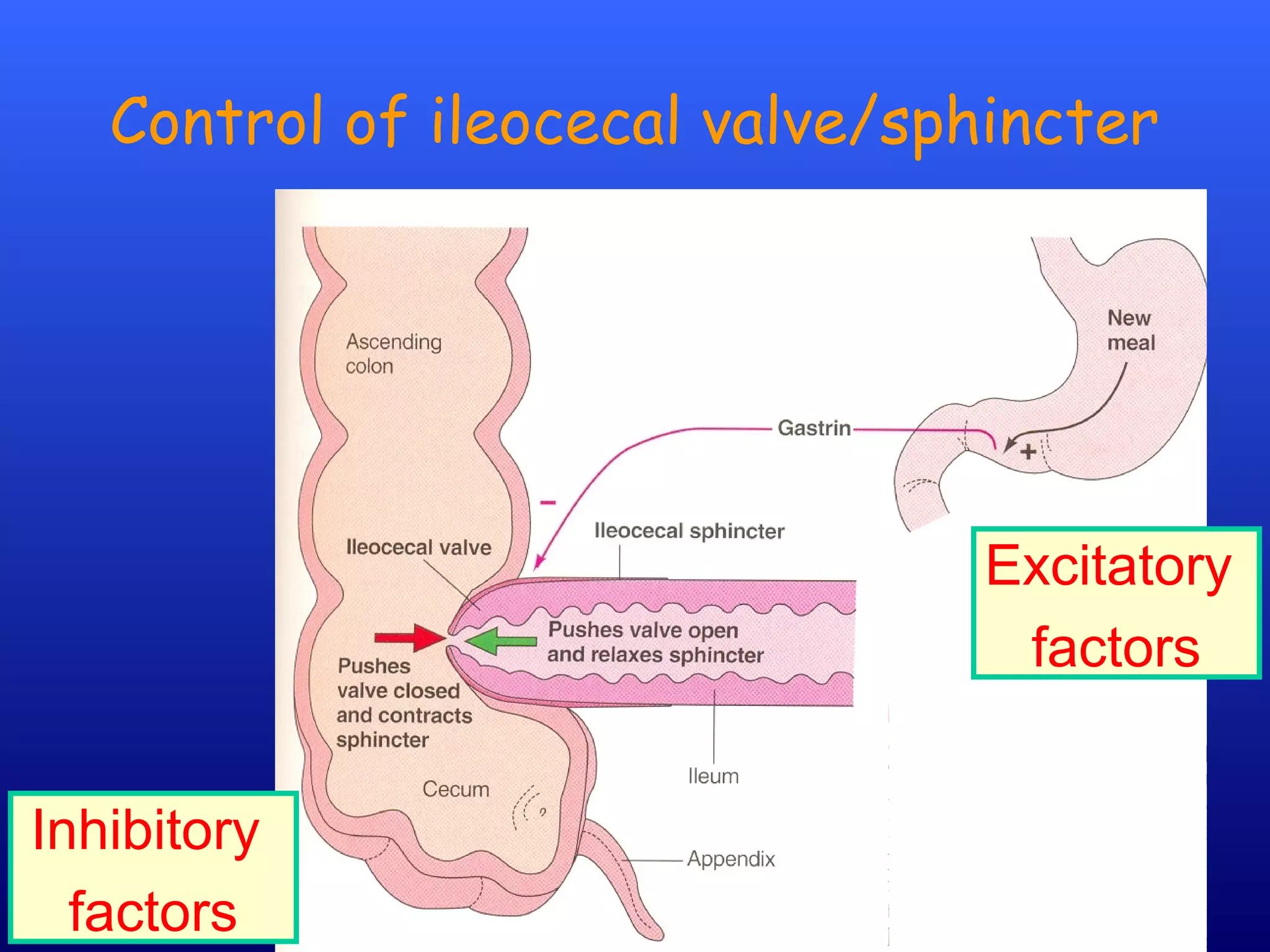
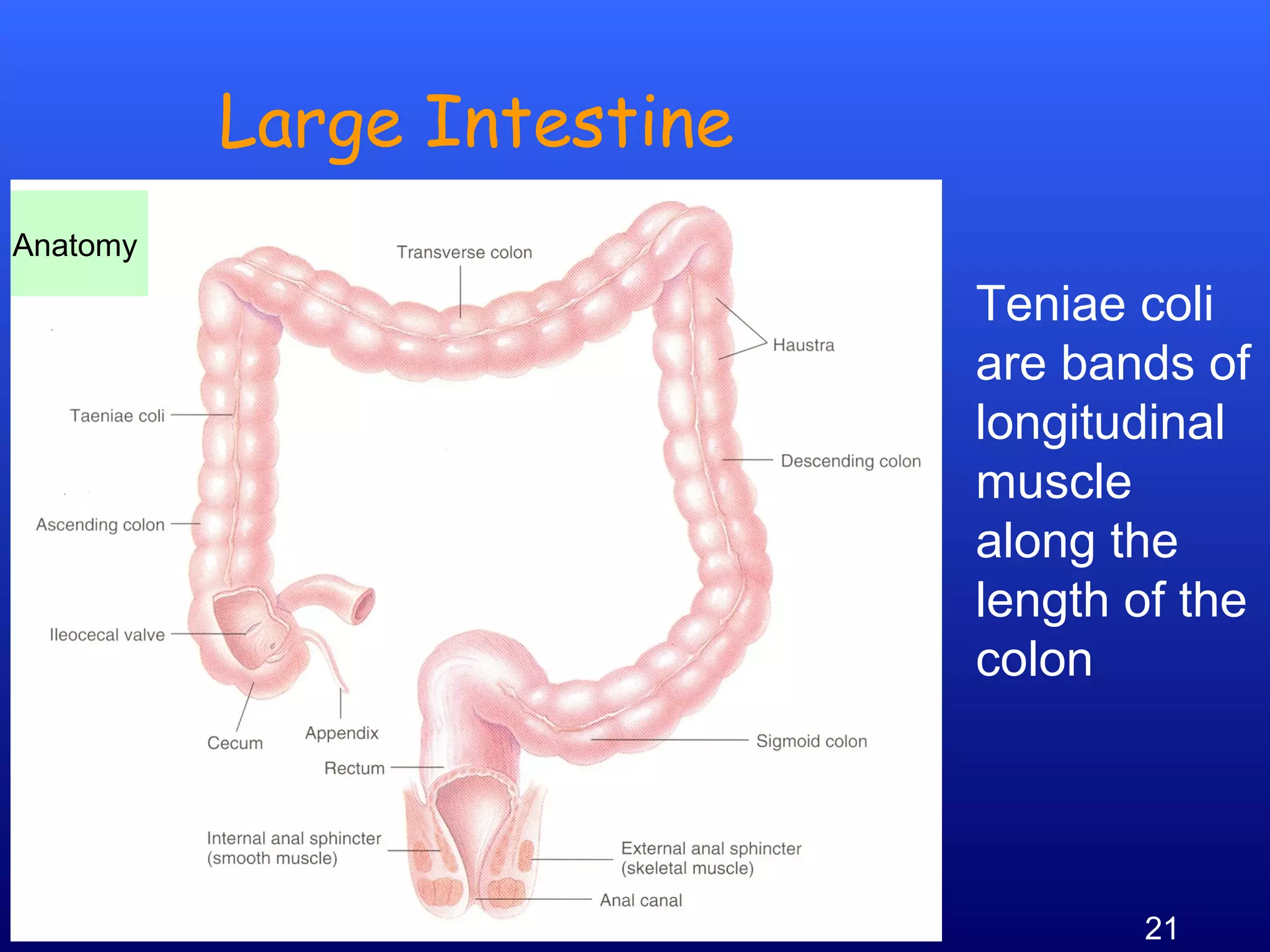
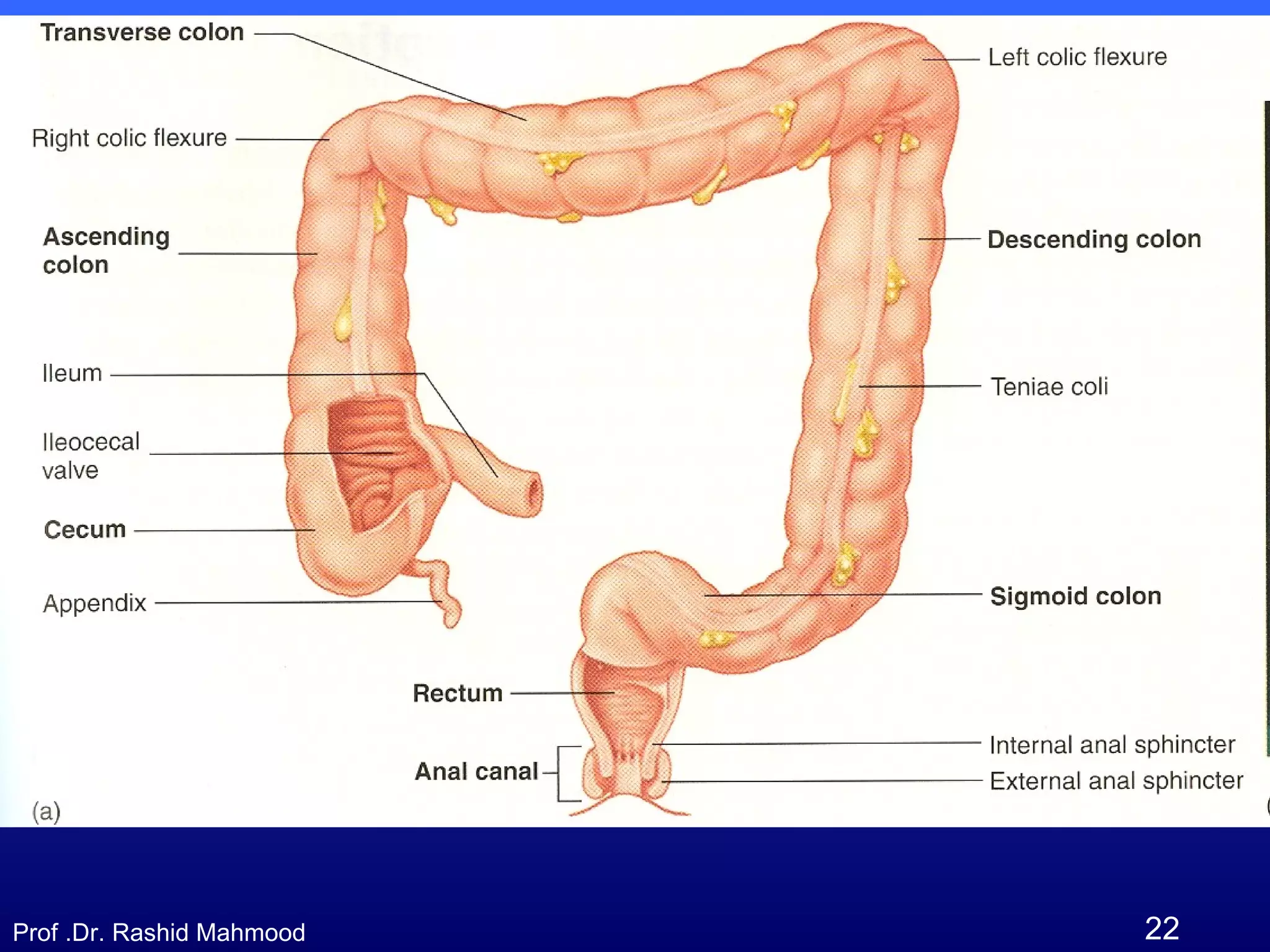
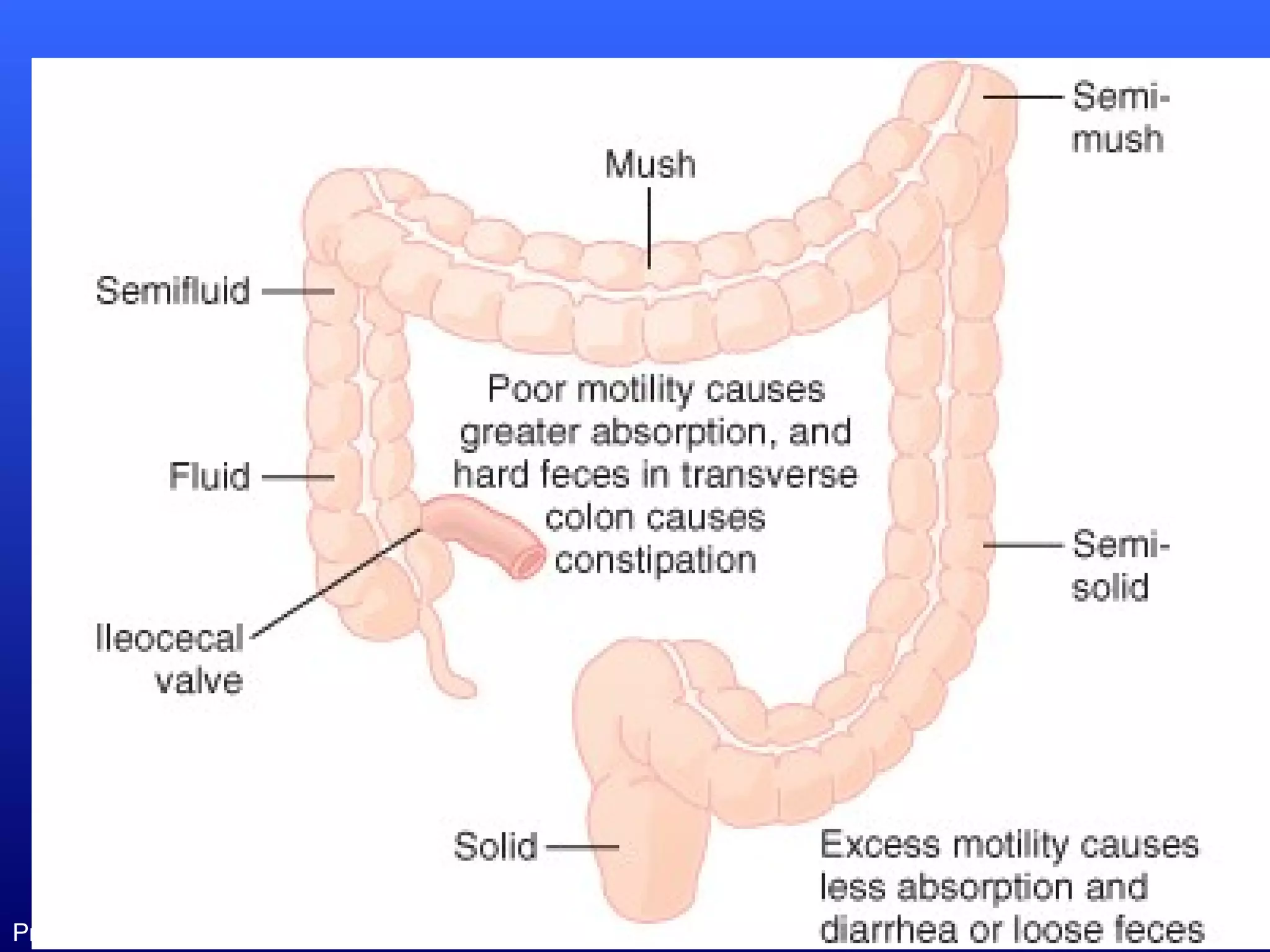
The document discusses the movements of the small and large intestines. It begins by describing two types of movements in the small intestine - mixing (segmentation) contractions and propulsive (peristalsis) movements. Nervous and hormonal factors that control peristalsis are discussed, including gastroenteric reflexes and hormones like gastrin and CCK. The document then covers the ileocecal valve and sphincter, which prevent backflow and allow controlled emptying. Finally, it describes two types of movements in the large intestine - mixing (haustration) movements proximally and propulsive (mass) movements distally.