Downloaded 43 times

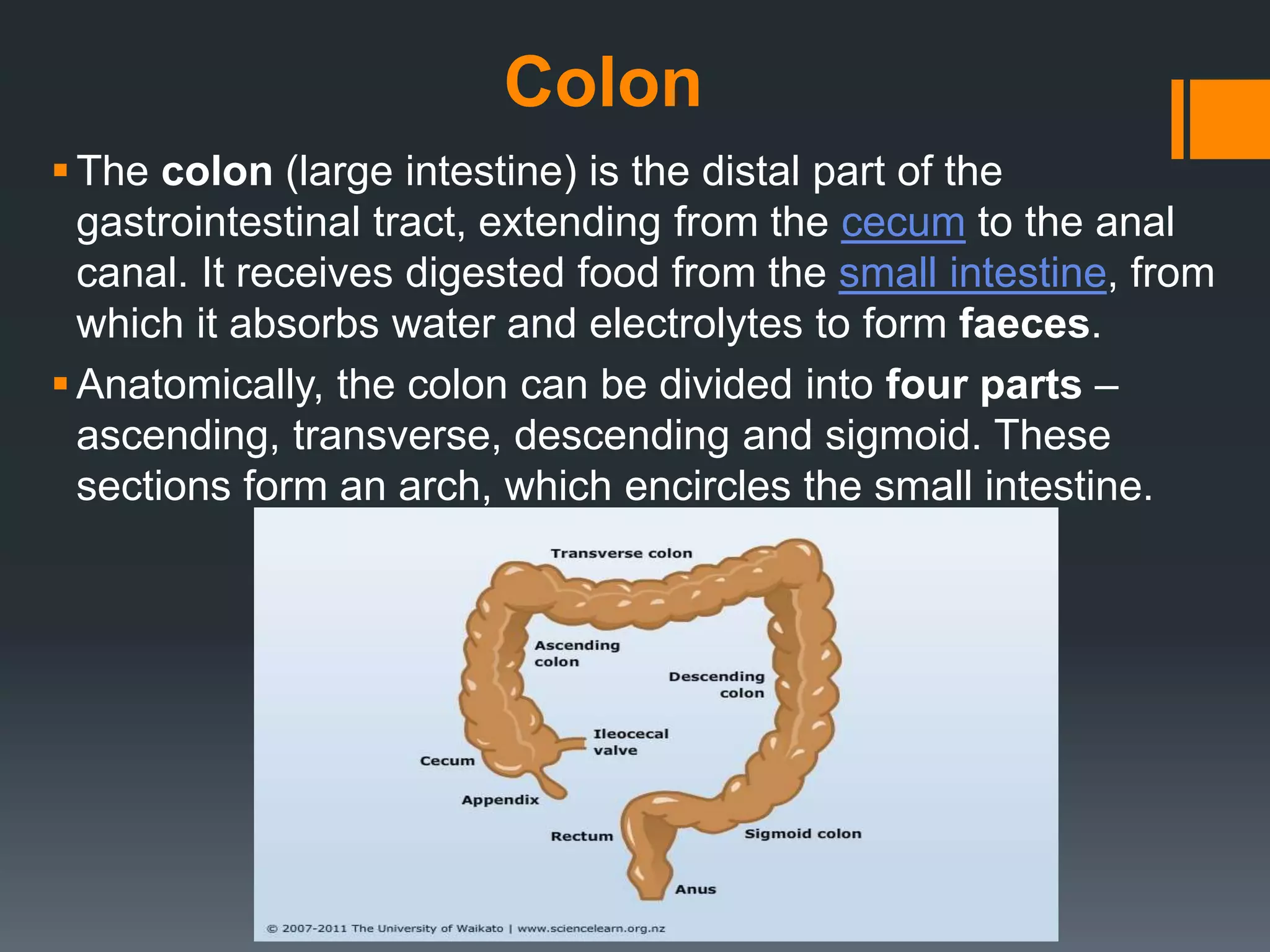


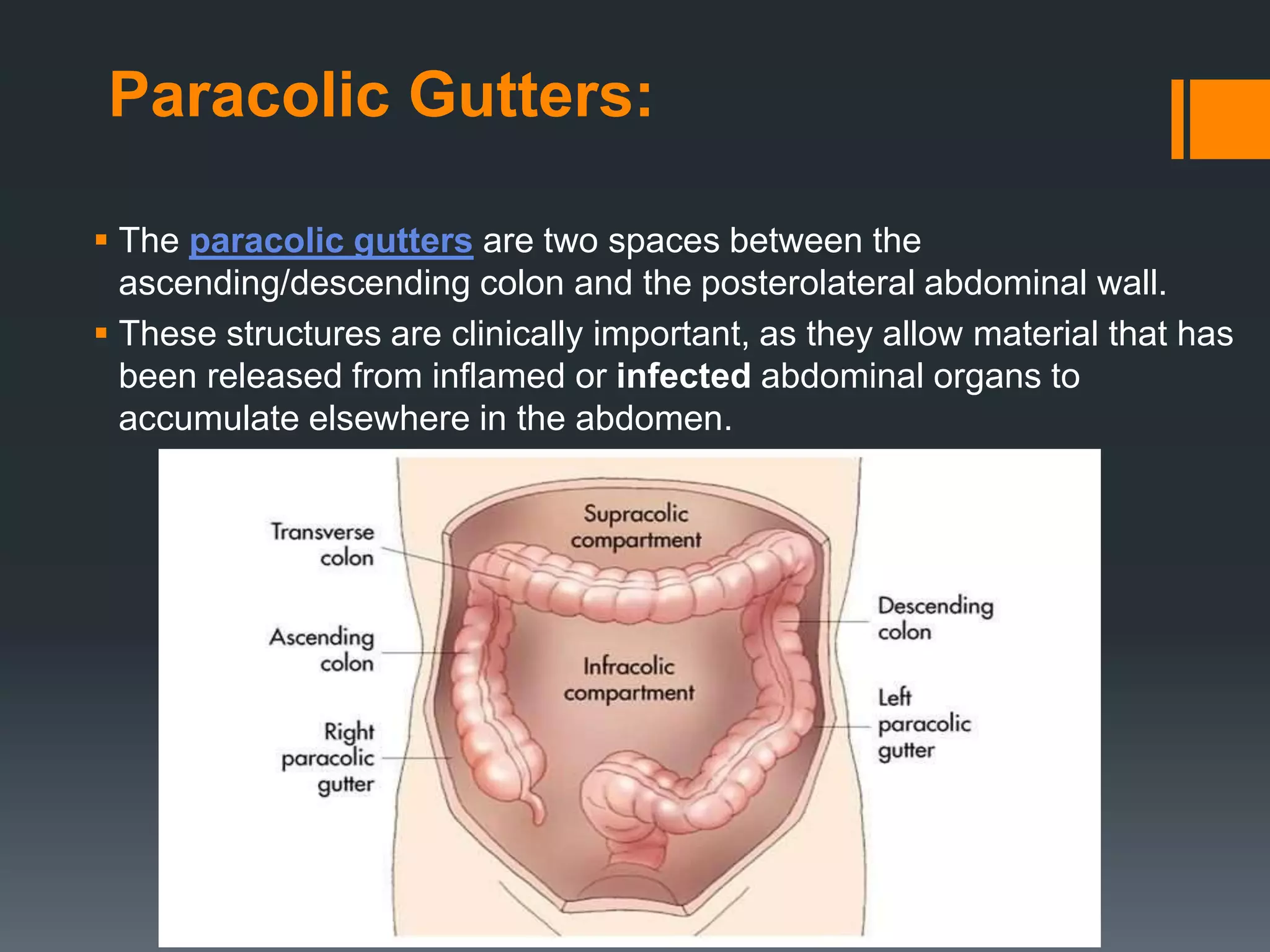











The large intestine extends from the small intestine to the anus. It is composed of the cecum, colon, and rectum. The colon can be divided into four parts - ascending, transverse, descending, and sigmoid. It absorbs water from digested food and forms feces. Diseases that can affect the large intestine include colorectal cancer, colonic polyps, ulcerative colitis, diverticulitis, and irritable bowel syndrome.



































































