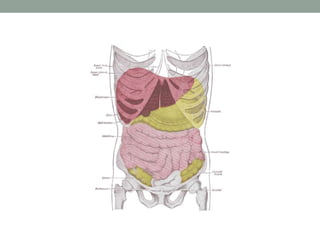
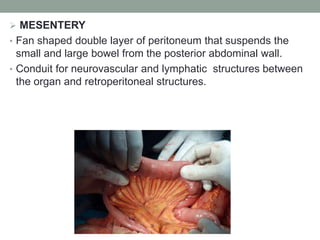
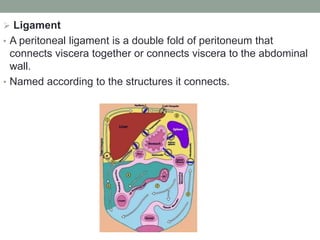
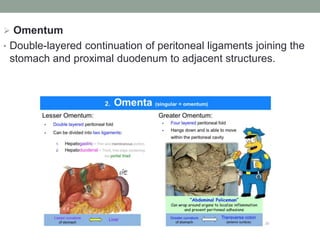
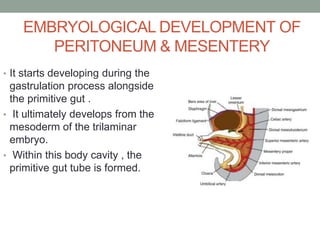
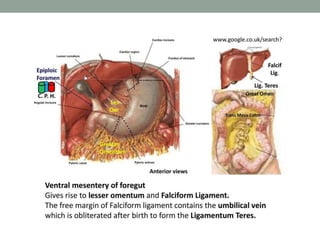
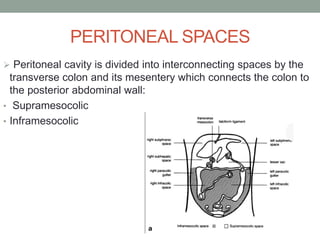
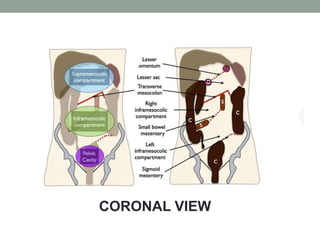
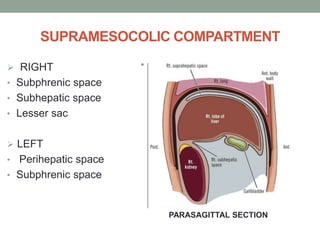
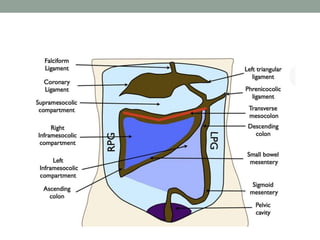
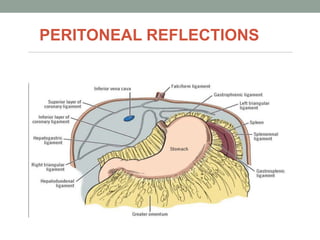
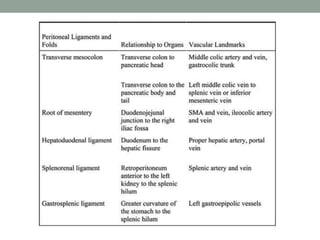
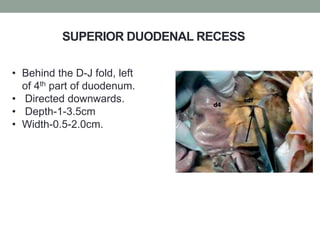
The peritoneum lines the abdominal cavity and comprises two layers. The mesentery suspends portions of the bowel and contains blood vessels, lymph nodes, and nerves. The peritoneal spaces include the lesser sac, supracolic and infracolic compartments. During development, the peritoneum and mesentery arise from the trilaminar embryo. Diseases can spread within the peritoneal cavity along ligaments, mesenteries, and lymphatics. The omentum, mesentery, and peritoneal recesses have clinical relevance for surgery and disease spread.