Download to read offline

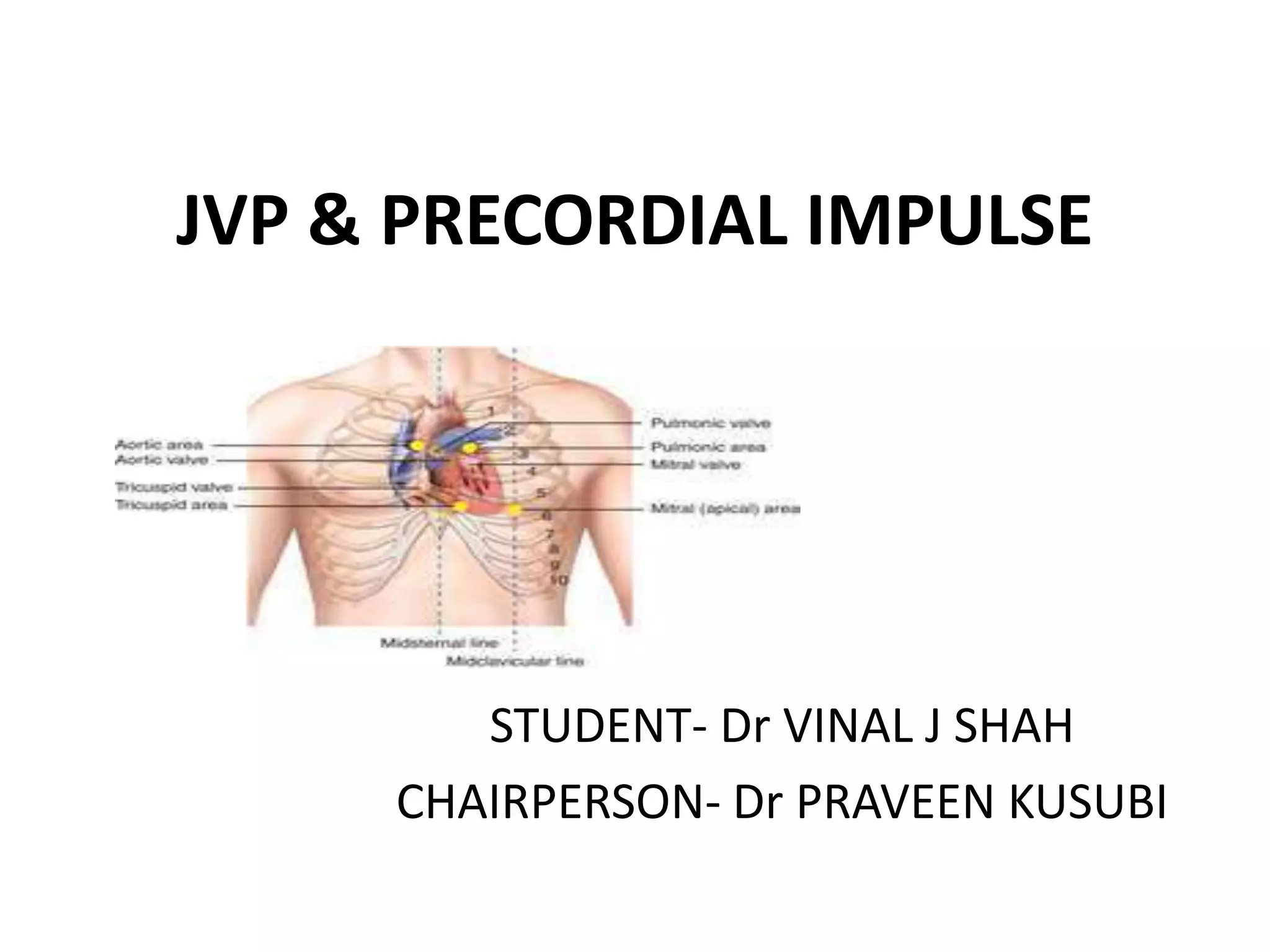
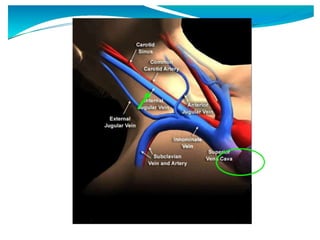
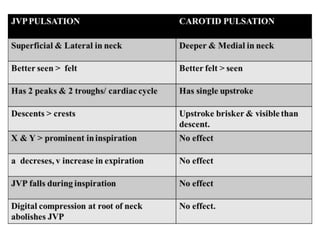
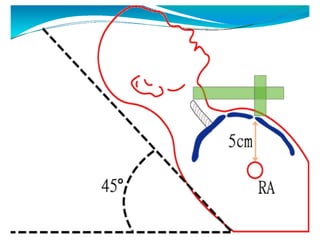
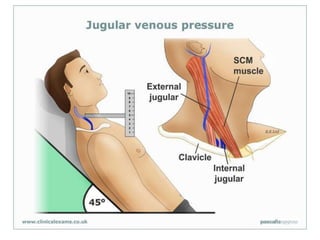

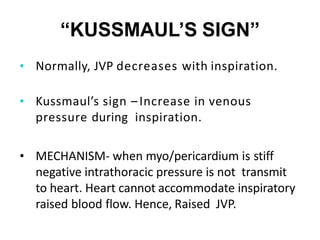



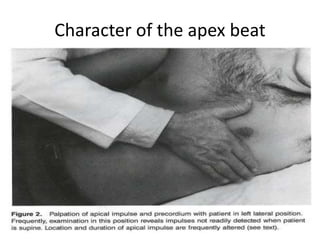
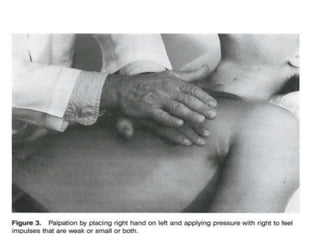
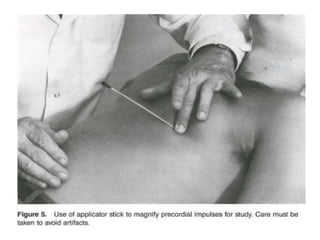



The document discusses jugular venous pressure (JVP) and precordial impulse, providing insights into their physiological significance, measurement techniques, and associated clinical implications. Key concepts include the anatomy of the jugular veins, variations in JVP, signs such as Kussmaul's sign, and methods for assessing the apical impulse as part of a cardiac examination. It emphasizes the importance of proper positioning and techniques for evaluating cardiovascular function and identifying abnormalities.














































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








