
Downloaded 17 times

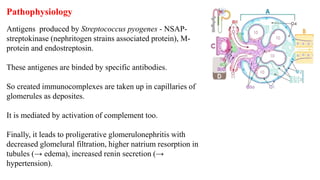
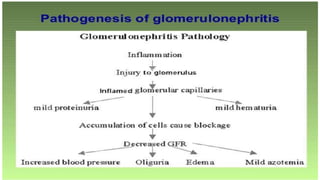
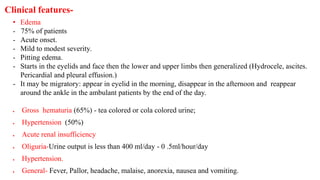
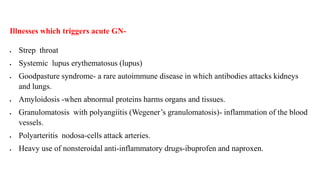

Poststreptococcal acute glomerulonephritis (AGN) is a common condition in childhood caused by a Streptococcus pyogenes infection. It involves an immune response that leads to inflammation of the glomeruli in the kidneys. Symptoms include edema, gross hematuria, hypertension, and acute renal insufficiency. Treatment focuses on controlling blood pressure, restricting fluid and salt intake, and administering antibiotics. While early AGN is often temporary and reversible, chronic glomerulonephritis can lead to permanent kidney damage if not properly managed.












































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










