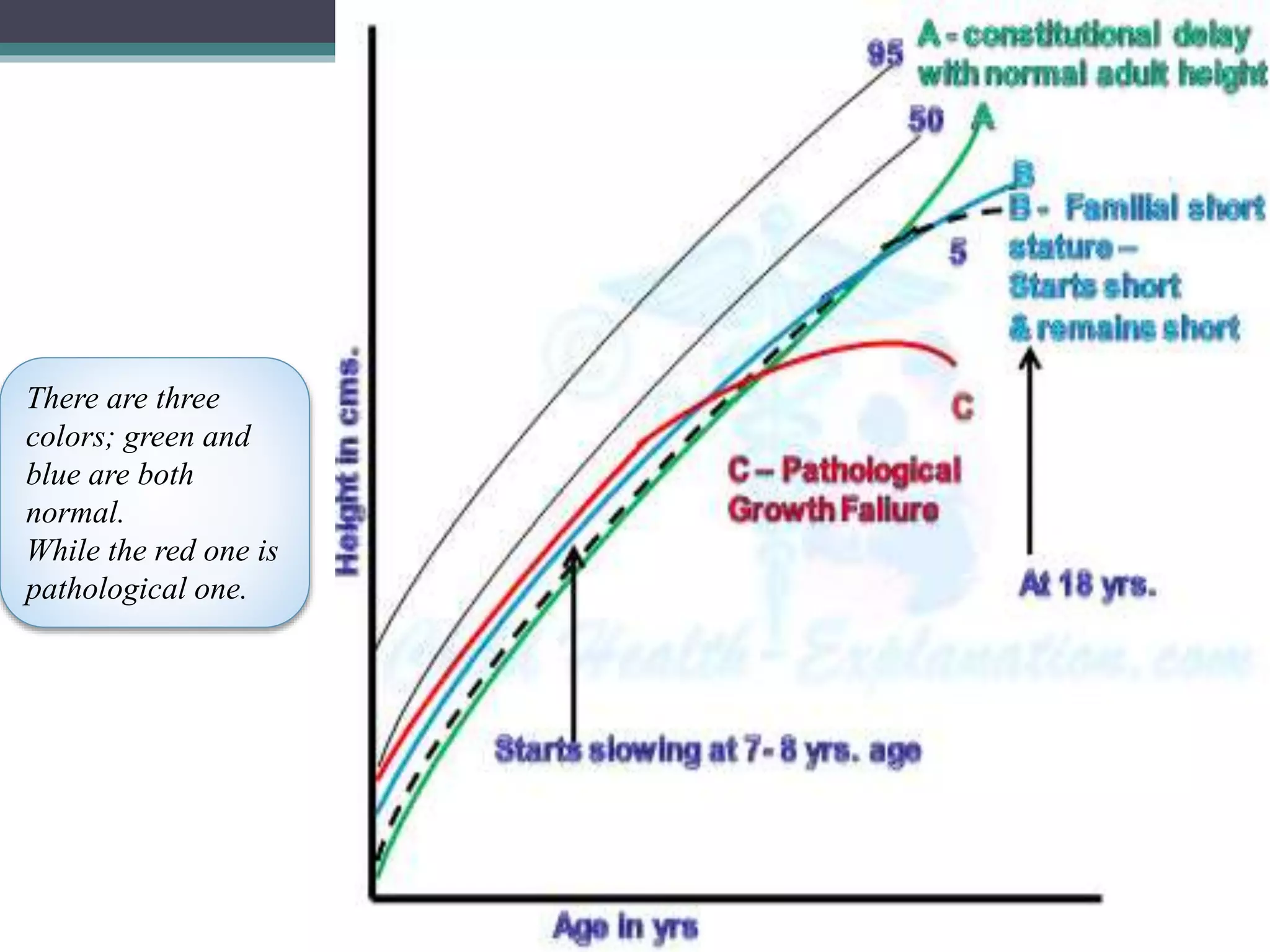
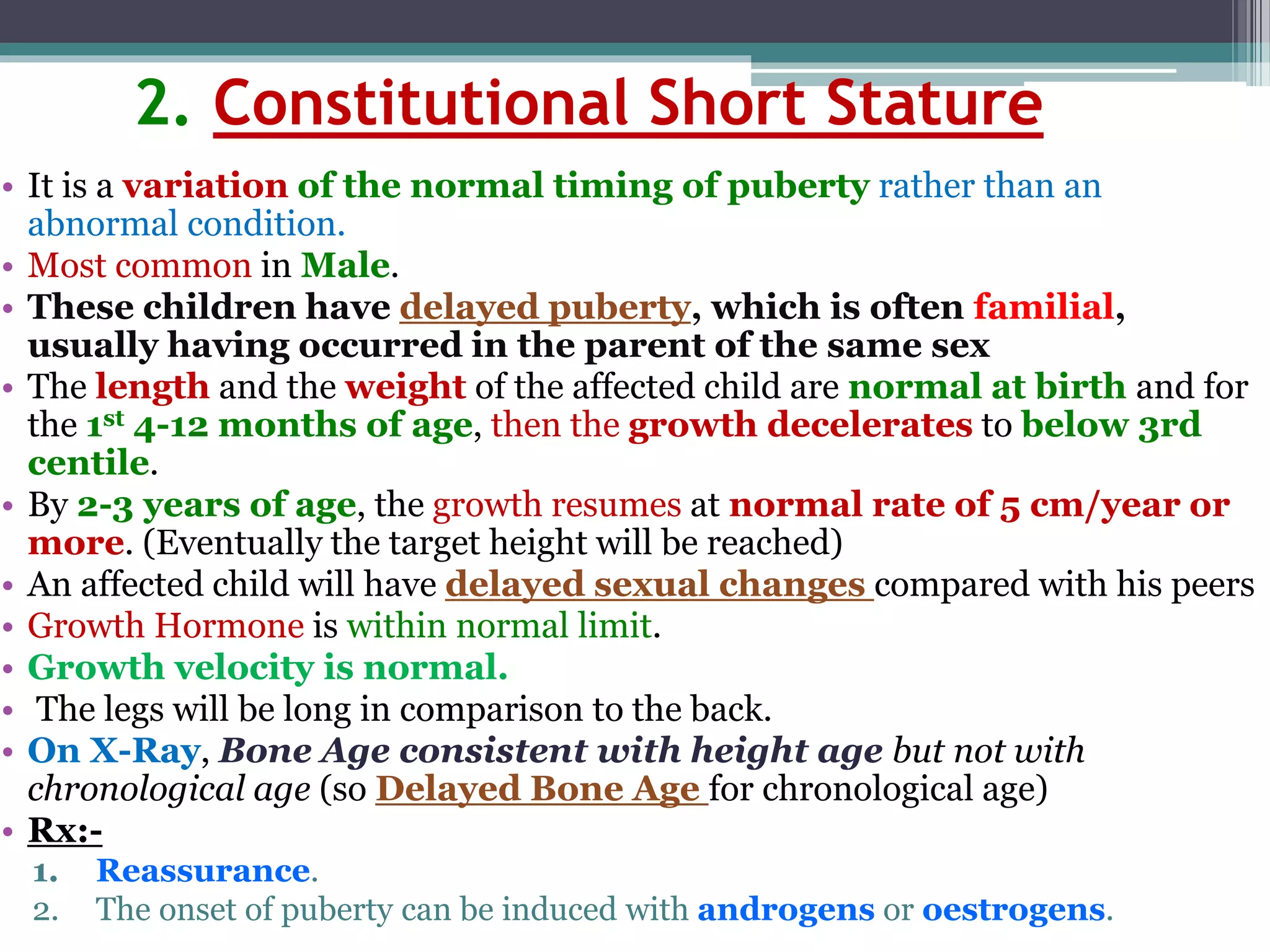
1. Short stature can be caused by familial, constitutional, or pathological factors. Familial short stature runs in families while constitutional short stature involves delayed puberty.
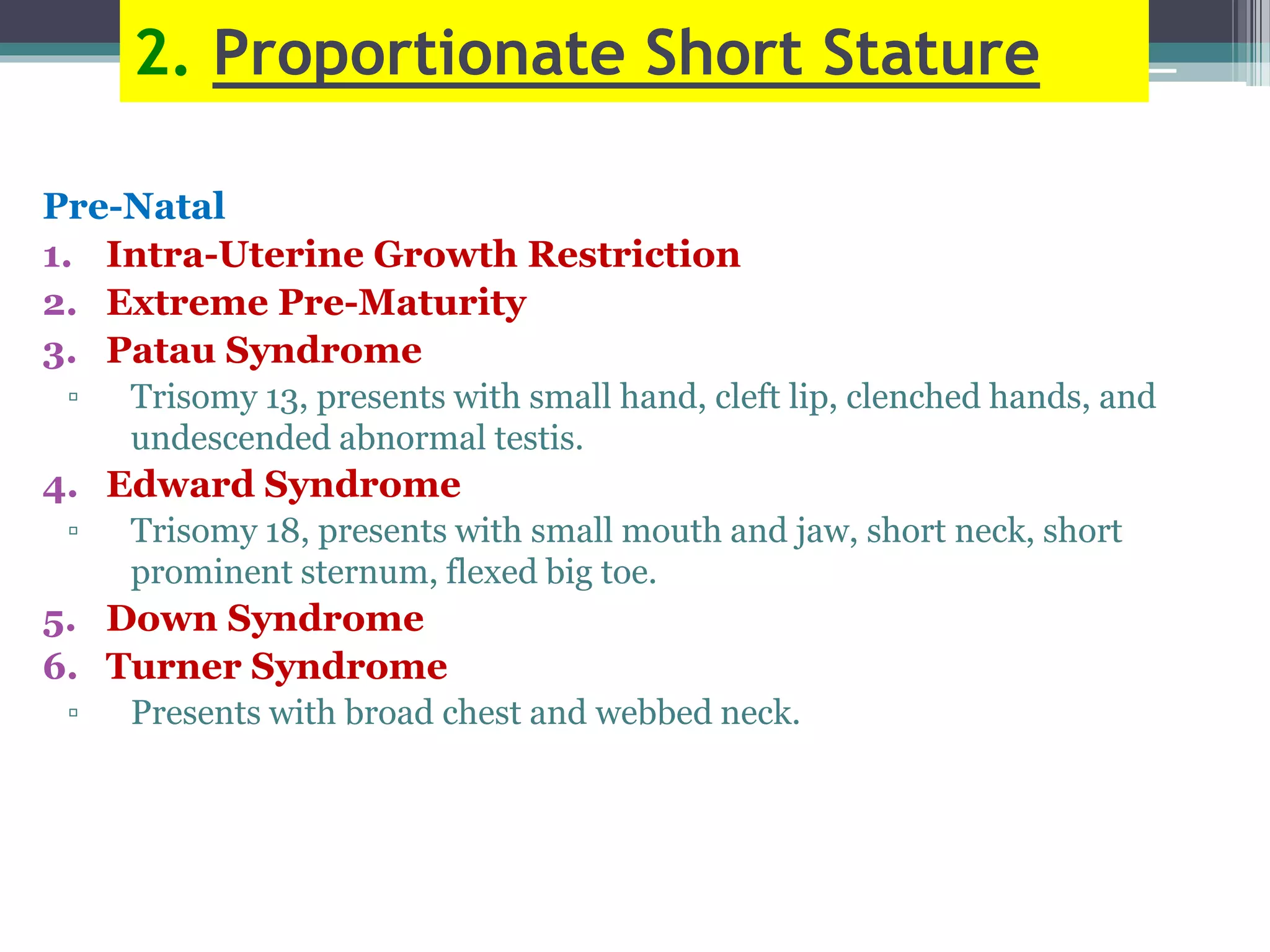
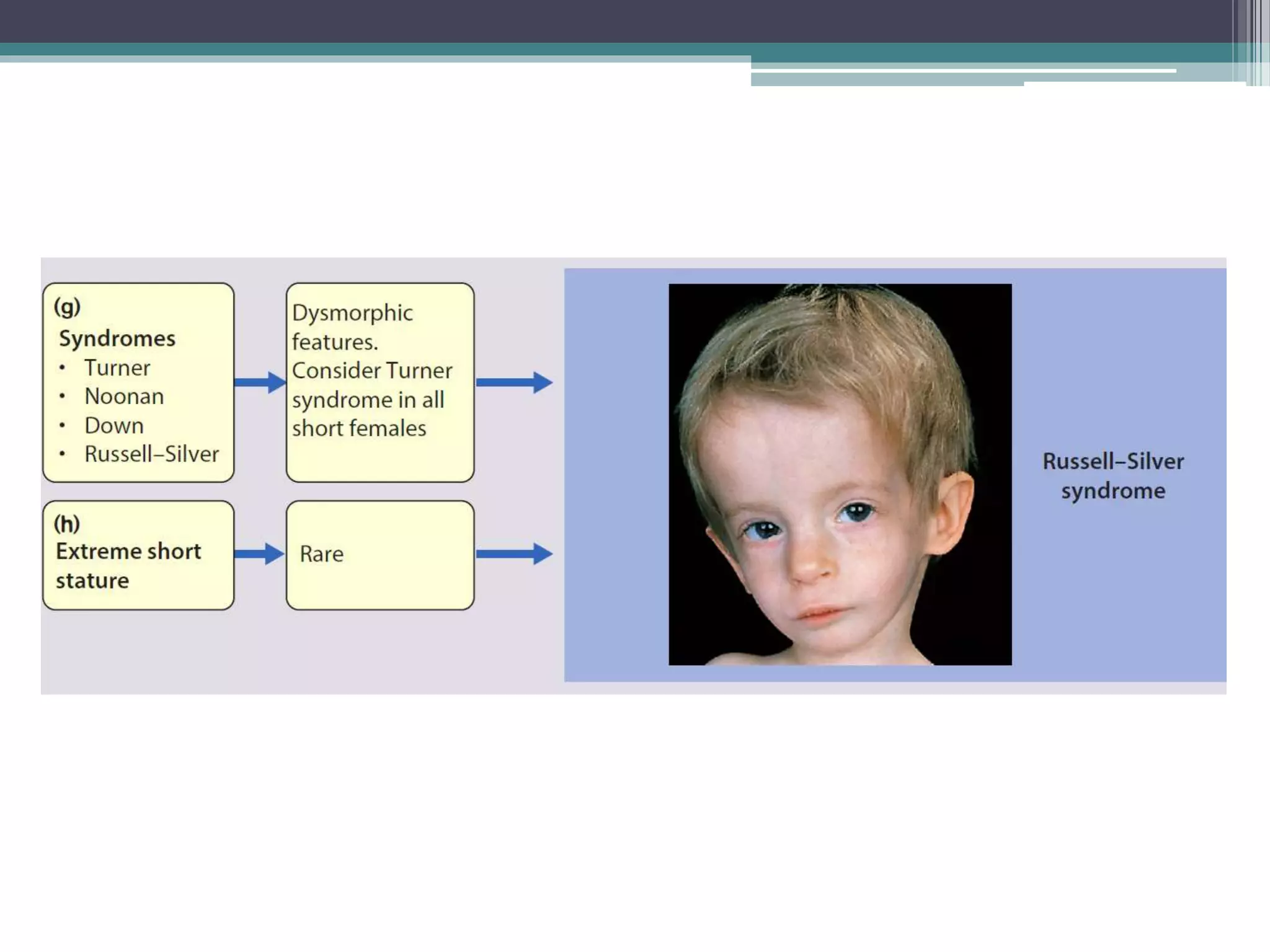
2. Pathological short stature can be disproportionate involving abnormal limb ratios, or proportionate involving prenatal issues like IUGR or postnatal diseases/nutritional disorders.
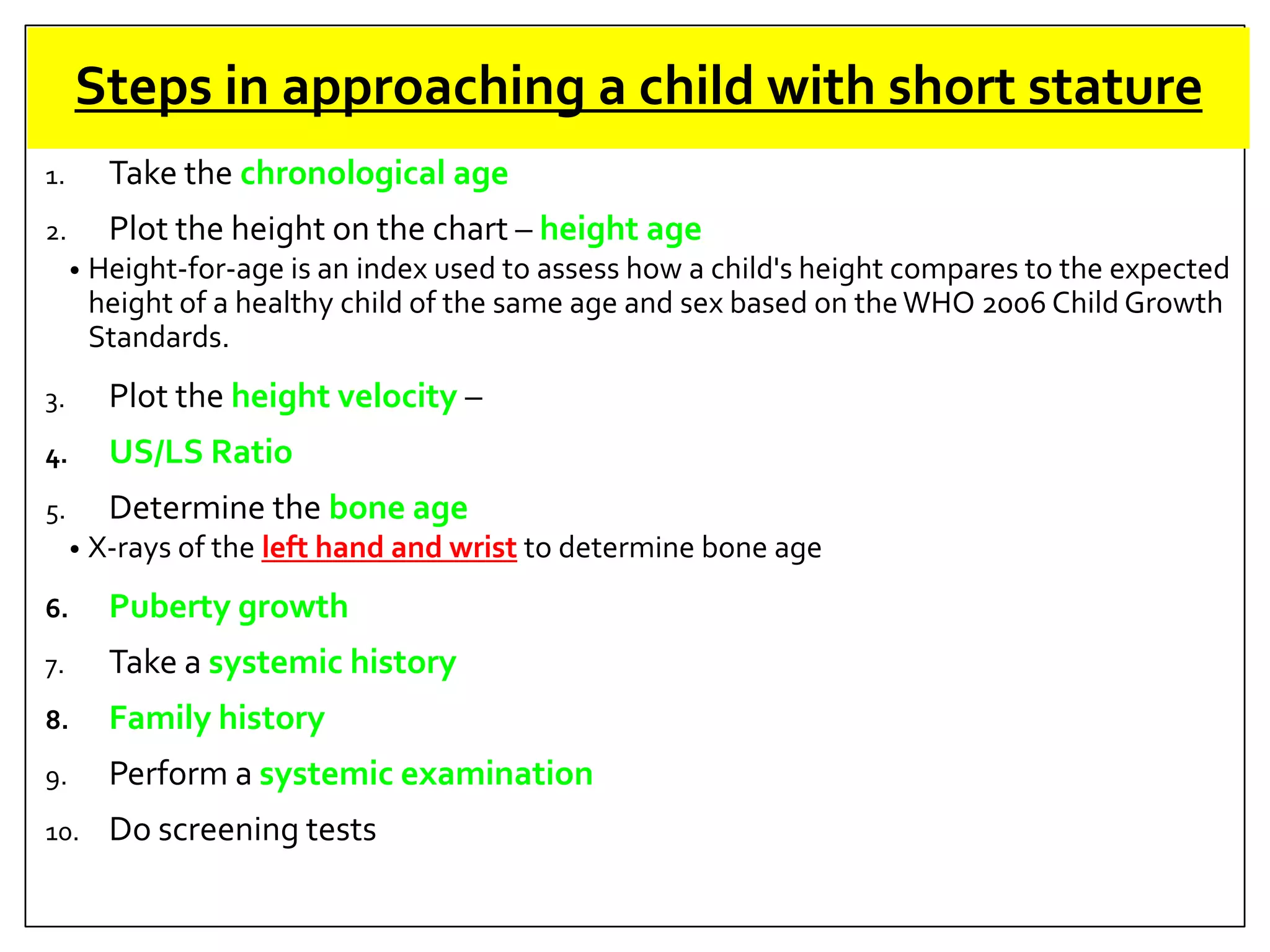
3. Evaluating a short child involves assessing growth charts, growth velocity, bone age, family history, and screening tests to classify the cause of short stature.