Downloaded 514 times

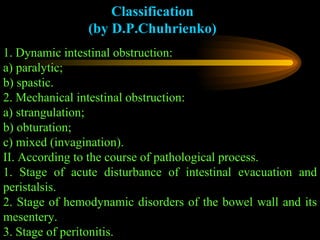
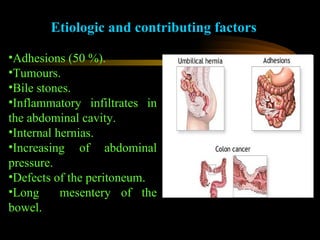

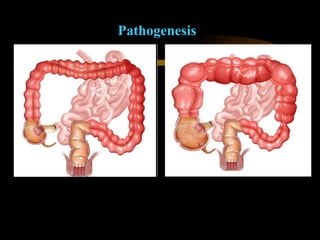














Intestinal obstruction is a complete or partial blockage of the intestines that can result from various causes. It occurs in approximately 9.4% of urgent abdominal cases and 1.2% of all surgical diseases. Causes include adhesions, tumors, bile stones, hernias, and inflammatory infiltrates. Symptoms depend on the level and type of obstruction but generally include acute pain, vomiting, nausea, stool and gas retention, and dehydration. Treatment involves conservative management for mild cases or surgery to remove the obstruction for more severe cases.



































































