Downloaded 21 times

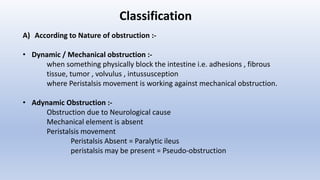
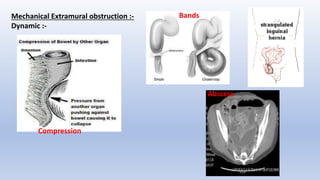
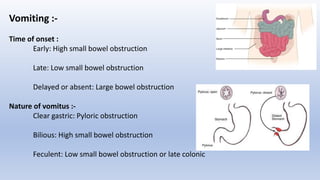
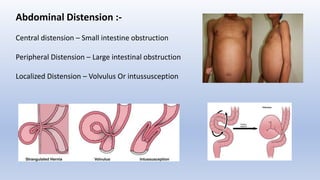
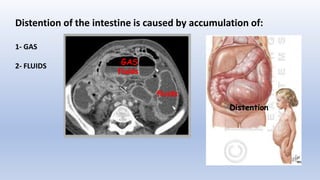
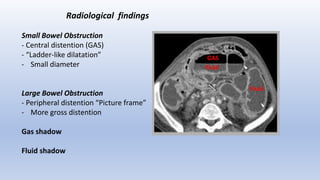


This document provides an overview of intestinal obstruction. It defines intestinal obstruction as a partial or complete blockage of the small or large intestine. It then classifies intestinal obstructions based on their nature, cause, severity, and blood supply. The most common causes of small and large intestine obstructions are also outlined. Clinical features, investigations, and treatment approaches for both conservative management and surgery are discussed. Key points include outlining signs of strangulation versus simple obstruction and indications for surgical intervention.


































































