Downloaded 56 times


















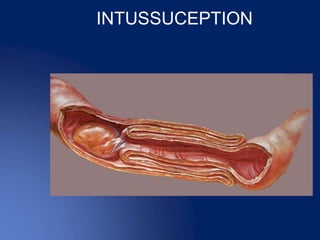































































This document discusses intestinal obstruction, including its definition, causes, clinical features, investigations and management. Intestinal obstruction occurs when bowel contents cannot pass through normally due to a mechanical or functional blockage. Clinical features depend on the location and cause of obstruction and may include pain, vomiting, distension and constipation.























































































