INTRODUCTION
• Intestinal obstructionstill is a challenging, commonly acute condition in surgical
practice.
• Adhesions are becoming the more common cause of intestinal obstruction
• Common causes for adhesions are gynecologic surgeries, appendicectomy,
colonic and pelvic surgeries.
• 20% cases of intestinal obstruction are due to malignancy or its peritoneal
carcinomatosis spread.
• More than 50% of intestinal obstruction in western countries are due to
adhesions
• 20% due to malignancies; 10-15% due to hernias.
• Crohn’s disease is also becoming a common cause of obstruction.
• Note:
• Adhesions and hernias are most common causes of intestinal obstruction
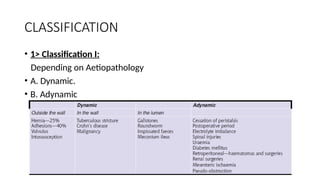
• 2> ClassificationII:
• Depending on Type of Obstruction
• 1. Acute: Common in small bowel.
• 2. Chronic.
• 3. Acute on chronic: Common in large bowel.
• 4. Closed loop obstruction.
DYNAMIC OBSTRUCTION
• Itis mechanical blockage of normal propulsion and passage of
intestinal contents.
• Obstruction may be
• external/internal
• partial (incomplete or subacute)/complete;
• acute/acute on chronic/or chronic;
• simple/closed loop/strangulation;
• congenital/acquired;
• proximal/distal.
8.
• Earlier, herniawas the commonest cause of intestinal
obstruction.
• Now adhesions (40%) are the commonest cause
• Recurrent obstruction is more common in adhesions.
• Adhesions commonly cause small bowel obstruction than
large bowel.
• 80% of intestinal obstruction occurs in small bowel; 20% in
colon.
• Colonic obstruction :
• 70% of colonic obstruction is due to malignancy.
• 30% is due to volvulus; diverticulitis, inflammatory cause
like tuberculosis, etc.
• Mortality
• 3% in obstruction without strangulation;
• 30% in obstruction with strangulation.
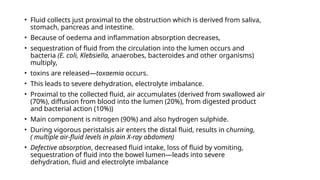
• Fluid collectsjust proximal to the obstruction which is derived from saliva,
stomach, pancreas and intestine.
• Because of oedema and inflammation absorption decreases,
• sequestration of fluid from the circulation into the lumen occurs and
bacteria (E. coli, Klebsiella, anaerobes, bacteroides and other organisms)
multiply,
• toxins are released—toxaemia occurs.
• This leads to severe dehydration, electrolyte imbalance.
• Proximal to the collected fluid, air accumulates (derived from swallowed air
(70%), diffusion from blood into the lumen (20%), from digested product
and bacterial action (10%))
• Main component is nitrogen (90%) and also hydrogen sulphide.
• During vigorous peristalsis air enters the distal fluid, results in churning,
( multiple air-fluid levels in plain X-ray abdomen)
• Defective absorption, decreased fluid intake, loss of fluid by vomiting,
sequestration of fluid into the bowel lumen—leads into severe
dehydration, fluid and electrolyte imbalance
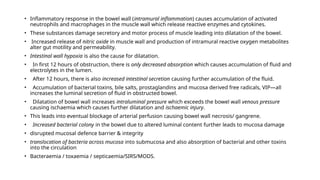
12.
• Inflammatory responsein the bowel wall (intramural inflammation) causes accumulation of activated
neutrophils and macrophages in the muscle wall which release reactive enzymes and cytokines.
• These substances damage secretory and motor process of muscle leading into dilatation of the bowel.
• Increased release of nitric oxide in muscle wall and production of intramural reactive oxygen metabolites
alter gut motility and permeability.
• Intestinal wall hypoxia is also the cause for dilatation.
• In first 12 hours of obstruction, there is only decreased absorption which causes accumulation of fluid and
electrolytes in the lumen.
• After 12 hours, there is also increased intestinal secretion causing further accumulation of the fluid.
• Accumulation of bacterial toxins, bile salts, prostaglandins and mucosa derived free radicals, VIP—all
increases the luminal secretion of fluid in obstructed bowel.
• Dilatation of bowel wall increases intraluminal pressure which exceeds the bowel wall venous pressure
causing ischaemia which causes further dilatation and ischaemic injury.
• This leads into eventual blockage of arterial perfusion causing bowel wall necrosis/ gangrene.
• Increased bacterial colony in the bowel due to altered luminal content further leads to mucosa damage
• disrupted mucosal defence barrier & integrity
• translocation of bacteria across mucosa into submucosa and also absorption of bacterial and other toxins
into the circulation
• Bacteraemia / toxaemia / septicaemia/SIRS/MODS.
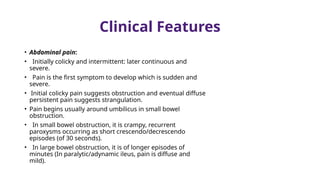
Clinical Features
• Abdominalpain:
• Initially colicky and intermittent: later continuous and
severe.
• Pain is the first symptom to develop which is sudden and
severe.
• Initial colicky pain suggests obstruction and eventual diffuse
persistent pain suggests strangulation.
• Pain begins usually around umbilicus in small bowel
obstruction.
• In small bowel obstruction, it is crampy, recurrent
paroxysms occurring as short crescendo/decrescendo
episodes (of 30 seconds).
• In large bowel obstruction, it is of longer episodes of
minutes (In paralytic/adynamic ileus, pain is diffuse and
mild).
16.
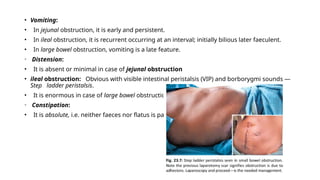
• Vomiting:
• Injejunal obstruction, it is early and persistent.
• In ileal obstruction, it is recurrent occurring at an interval; initially bilious later faeculent.
• In large bowel obstruction, vomiting is a late feature.
• Distension:
• It is absent or minimal in case of jejunal obstruction
• ileal obstruction: Obvious with visible intestinal peristalsis (VIP) and borborygmi sounds —
Step ladder peristalsis.
• It is enormous in case of large bowel obstruction.
• Constipation:
• It is absolute, i.e. neither faeces nor flatus is passed.
17.
• Dehydration:
• Leadsto oliguria , renal failure.
• Features of toxemia and septicemia:
• Tachycardia, tachypnoea, fever, sunken eyes, cold periphery.
• Abdominal tenderness:
• It is initially localized but later becomes diffuse—is a feature of intestinal
obstruction.
• Rebound tenderness and guarding will not be present in simple obstruction
which are features of strangulation.
• Features of strangulation:
• Continuous severe pain, shock, tenderness, rebound tenderness (Blumberg’s
sign).
• Guarding and rigidity, absence of bowel sounds.
• In case of strangulated hernia, a swelling which is tense, tender, rigid,
irreducible, no expansile impulse on coughing and history of recent increase
in size is seen.
18.
• Temperature:
• Feversignifies inflammation in the bowel wall/ ischaemia/perforation.
• Hypothermia can occur when septicemia develops due to lack of
pyrogenic response.
• It suggests poor prognosis.
• Bowel sounds:
• They are increased—high pitched metallic (rushes and groans) sounds
followed by metallic tinkling sounds of dilated bowel.
• Eventually once fatigue occurs or gangrene develops, bowel sounds are
not heard—silent abdomen of peritonitis develops
• (In paralytic ileus, there are only continuous metallic sounds of dilated
bowel).
• Per-rectal examination:
• Shows empty, dilated rectum, often with tenderness.
• If rectal growth is the cause for obstruction, it may be palpable.
19.
INVESTIGATIONS
• Plain X-rayabdomen:
• (initially supine abdominal X-ray is taken; later if needed X-ray in erect posture is
taken if perforation is suspected).
• Multiple air-fl uid levels.
• Proximal the obstruction >>>>>>> Lesser the air fluid level.
• Distal the obstruction >>>>>>>>> More the air fluid level.
• Normally, three fluid levels can be seen in plain X-ray fIlm—at fundus of stomach, at
duodenum and often at caecum.
• Jejunum shows concertina effect due to valvulae conniventes (Herring bone pattern)
—by the valves of Kerckring.
• Ileum is smooth and characterless (by Wangensteen).
• Large bowel shows haustration.
• Pneumobilia (gas in biliary tree) may be due to gallstone ileus.
20.
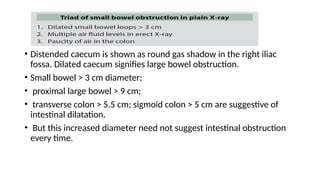
• Distended caecumis shown as round gas shadow in the right iliac
fossa. Dilated caecum signifies large bowel obstruction.
• Small bowel > 3 cm diameter;
• proximal large bowel > 9 cm;
• transverse colon > 5.5 cm; sigmoid colon > 5 cm are suggestive of
intestinal dilatation.
• But this increased diameter need not suggest intestinal obstruction
every time.
22.
• Barium (microbar solution) enema or gastrografiN contrast enema X-ray is useful in
intussusception.
• [Barium meal is usually contraindicated in acute intestinal obstruction. ]
• However dilute (micro bar) barium meal/ gastrografin meal follow through X-ray may be done with
caution in suspected subacute/partial intestinal obstruction under fluoroscopy,
• Otherwise it may precipitate complete obstruction or perforation and barium peritonitis which is very
dangerous
• US abdomen
• dilated bowel and fluid in the peritoneal cavity.
• It is better than X-ray but not as good as CT scan.
• It has got 95% sensitivity; 80% specificity; 80% accuracy.
• Doppler US is useful in detecting strangulation.
• CT scan
• It has got 93% sensitivity; 94% accuracy and 100% specificity.
• In CT scan small bowel loop > 2.5 cm suggests dilatation.
• It can show dilated loop, transition zone and collapsed part which are definitive features of intestinal
obstruction.
• It can also give idea of changes in the bowel wall, ischemia, strangulation, mesenteric oedema and
thickening.
• It also shows bowel wall gas, portal venous gas and mass lesion
23.
TREATMENT
• Nasogastric aspiration:
•To reduce toxic effects
• to reduce bowel distension which indirectly improves pulmonary
ventilation and to reduce possibility of aspiration pneumonia.
• Replacement of fluid and electrolytes.
• Antibiotics: Ampicillin, gentamycin, metronidazole, cephalosporins.
• Blood transfusion: FFP or platelet transfusions are often needed in
critical patient.
• ICU critical care: Systemic management of complications like ARDS, DIC,
SIRS are important.
• If there is hypotension, dopamine/dobutamine are also needed.
• CVP for fluid and monitoring: PCWP (pulmonary capillary wedge
pressure) monitoring are often needed in haemo dynamically unstable
patient.
24.
SURGERY
• Immediate laparotomy
•SITE OF OBSTRUCTION finding the junction of dilated proximal and collapsed distal bowel
• Cause of the obstruction is identified.
• The obstruction is relieved.
26.
IMPORTANT POINTS INSURGERY
• Warm saline soaked mop is placed over the doubtful area with 100%
oxygen inhalation for 20 minutes;
• if colour becomes normal with peristalsis then bowel is viable.
• On table Doppler study may be useful.
• Fluorescein fluorescence study may be helpful on table to check the
viability.
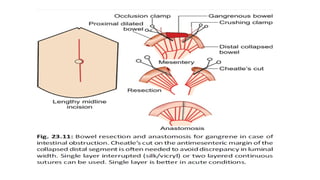
• If bowel is not viable resection and anastomosis is done.
• A good peritoneal wash is given and the abdominal cavity is drained.
• Abdomen is closed in layers using nonabsorbable sutures (polyethylene,
polypropylene, nylon).
• Often tension sutures are required.
• Small bowel can be decompressed using Savage’s decompressor.
27.
• Right-sided colonicobstruction, right hemicolectomy with ileocolic anastomosis is done.
• Left-sided colonic obstruction, left hemicolectomy(resection) and colo-colic anastomosis is
done with a defunctioning colostomy (right-sided transverse) which is closed after 6 weeks.
• Obstruction due to rectosigmoid growth with patient .
• Hartmann’s operation
• distal stump , after removal of the growth is closed, proximal colon is brought out as end
colostomy.
• Second look operation may be needed in doubtful cases or multiple segment obstructions in
24-48 hours to confirm viability.
• Laparoscopic approach may be useful in partial obstruction, proximal obstruction,
obstruction due to band. Conversion when needed should be done without hesitation.
• Acute postoperative obstruction
• CT is very useful.
• Initially it is treated conservatively (90%)
• suspected ischaemic cases or persistent obstruction becomes an indication for surgery.
• Resection with exteriorization may be the choice.

![• Barium (micro bar solution) enema or gastrografiN contrast enema X-ray is useful in
intussusception.
• [Barium meal is usually contraindicated in acute intestinal obstruction. ]
• However dilute (micro bar) barium meal/ gastrografin meal follow through X-ray may be done with
caution in suspected subacute/partial intestinal obstruction under fluoroscopy,
• Otherwise it may precipitate complete obstruction or perforation and barium peritonitis which is very
dangerous
• US abdomen
• dilated bowel and fluid in the peritoneal cavity.
• It is better than X-ray but not as good as CT scan.
• It has got 95% sensitivity; 80% specificity; 80% accuracy.
• Doppler US is useful in detecting strangulation.
• CT scan
• It has got 93% sensitivity; 94% accuracy and 100% specificity.
• In CT scan small bowel loop > 2.5 cm suggests dilatation.
• It can show dilated loop, transition zone and collapsed part which are definitive features of intestinal
obstruction.
• It can also give idea of changes in the bowel wall, ischemia, strangulation, mesenteric oedema and
thickening.
• It also shows bowel wall gas, portal venous gas and mass lesion](https://image.slidesharecdn.com/intestinalobstructionpathophycause-251204091600-0fedd230/85/Intestinal-obstruction-its-pathophysiology-and-causes-22-320.jpg)


































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













