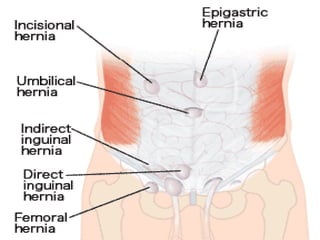
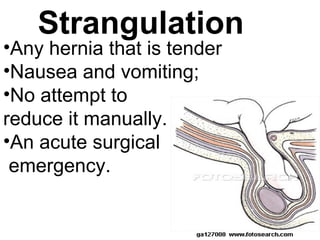
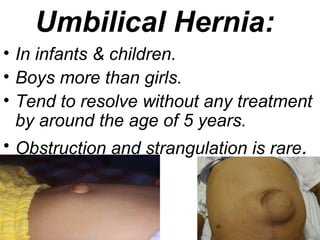
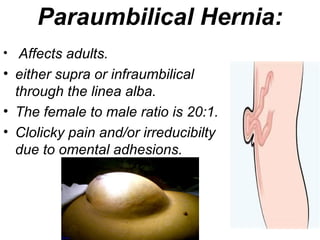
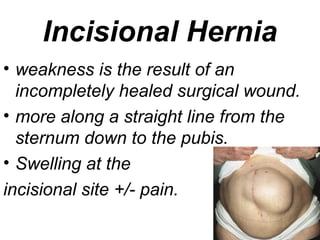
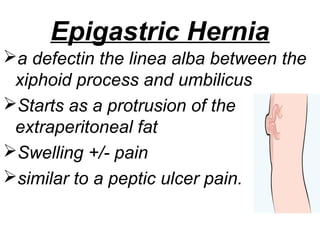
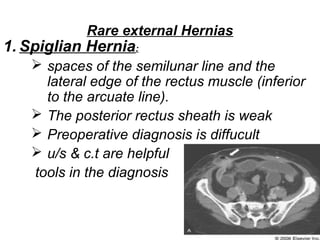
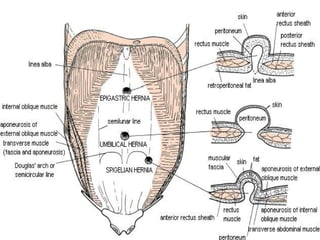
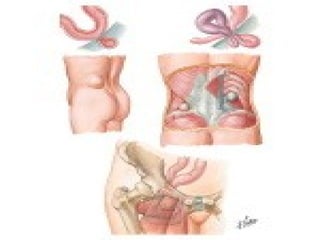
1. The document discusses different types of hernias, including inguinal, femoral, umbilical, incisional, and rare types.
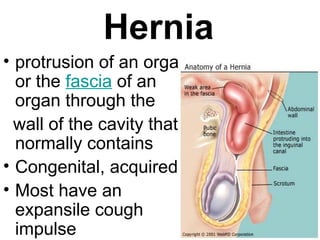
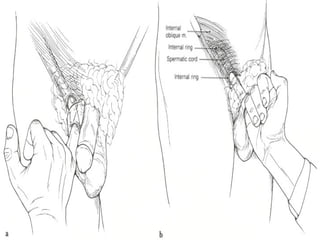
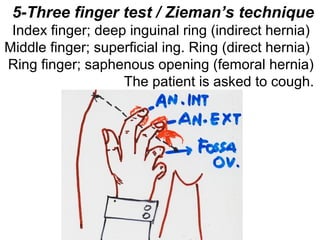
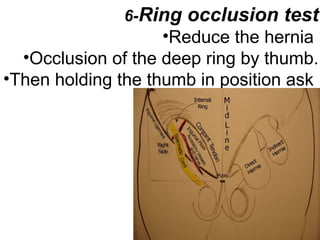
2. It provides details on examining patients for hernias, such as observing for visible lumps, checking for cough impulse, and performing reducibility tests.
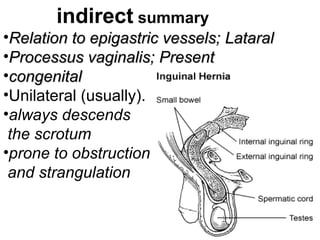
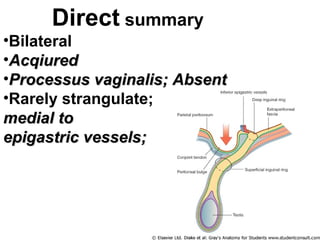
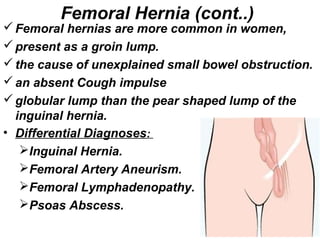
3. Key factors are described for differentiating between direct and indirect inguinal hernias, as well as differentiating inguinal from femoral hernias based on location and examination findings.

![Ingiunal canal Boundaries
MALT: 2M 2A, 2L, 2T:
Superior wall [roof]: 2 Muscles:
• Internal oblique Muscle
• Transverse abdominus Muscle
Anterior wall: 2 Aponeuroses:
• Aponeurosis of external oblique
• Aponeurosis of internal oblique
Lower wall [floor]: 2 Ligaments:
• Inguinal Ligament
• Lacunar Ligament
Posterior wall: 2Ts:
• Transversalis fascia [laterally]
• Conjoint Tendon [medially]](https://image.slidesharecdn.com/9hernia-130718004923-phpapp01/85/9-hernia-7-320.jpg)

































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


