Downloaded 143 times

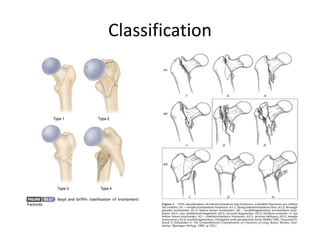


Intertrochanteric fractures are common hip fractures seen in the elderly that occur between the greater and lesser trochanters. There is no consensus on the best treatment, but options include intramedullary nails, sliding hip screws with side plates, and hemiarthroplasty in some cases. While both operative and non-operative treatments can be used, surgery typically leads to better outcomes through earlier mobilization and weight bearing. Newer intramedullary nails may provide faster recovery of walking ability compared to sliding hip screws, though implant selection depends on the fracture pattern and stability.


















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










