Thesis protocol
presentation
Thesis guide:-Dr. Manjeet Singh
Co guide:- Dr. Rakesh Gautam
Presented by:- Dr. Eshaan singh saini
Department of orthopaedics,
Adesh medical college and hospital, Kurukshetra
2.
TOPIC
COMPARISION OF TWINSCREW
DEROTATION TYPE VS SINGLE HELICAL
BLADE TYPE CEPHALOMEDULLARY
NAIL IN MANAGEMENT OF
INTERTROCHANTERIC FRACTURE
3.
Introduction
• Proximal femuror hip fractures remains the most common
reason for an elderly person to be admitted to an
orthopaedic ward. These fracture are relatively common in
elderly in fifth decade of life due to decreasing bone stock
leading to fracture by trivial trauma, thus, necessitating
hospital admission. Younger age group is getting involved
because of high energy trauma, rapid industrialisation
resulting in complex pattern of injury. Proximal femur
fracture occur 2 to 3 times more than female than males.
The risk of suffering from proximal femur fracture doubles
every 10 years after the age of 50 years.
4.
Why surgery isneeded for IT fractures?
• In Intertrochanteric fractures, since the bone is cancellous with
abundant muscle tissue around the fracture, the union is the rule,
unlike intracapsular fractures. The mostcommon complication
encountered in these fractures is malunion. Non-union is also very rare.
• Internal fixation is the treatment of choice for treating Intertrochanteric
fractures of the femur not because they fail to unite by conservative
treatment but because:
• 1. To obtain the best possible reduction (to avoid malunion).
• 2. To get the patient out of bed as soon as possible and thereby reduce
the complications associated with prolonged recumbency.
5.
Review of literature
•Sharan Mallya et al in 2019 Conducted a study on Comparison of radiological and functional outcome of unstable
intertrochanteric femur fractures treated using PFN and PFNA-2 in patients with osteoporosis Seventy-eight patients
with unstable intertrochanteric fractures and Singh's index < 3 were included. Twelve patients in PFNA2 group and 14
Patients in PFN group had sub-optimal implant position as per Cleveland index. The difference in neck shaft angle
between uninjured and operated side was more than 10° in four patients of PFNA2 group and seven patients of PFN
group. The average Harris hip score was 74.55 for PFNA2 group and 69.88 for PFN group. Four complications were
seen in PFNA2 group and 5 in PFN group. The functional outcome (p = 0.102) achieved with both the implants was
similar.
• Rong-Hua Tianet al in 2020 Conducted a study on Comparison of two methods of locating proximal femoral nail
anti-rotation in the treatment of femoral intertrochanteric fractures i.e. To compare the efficacy of three-point locating
versus routine locating techniques for implanting helical blades for proximal femoral nail anti-rotation-II in the
treatment of trochanteric fractures. All operations were performed by the same group of surgeons using proximal
femoral nail anti-rotation (PFNA); the helical blade was inserted into the femoral neck with the three-point locating
technique or by the usual method according to treatment group. Several figures including total operation time, elapsed
time for implanting the helical blade, intraoperative blood loss, X-ray exposure time, and tip-apex distance (TAD)
were measured and compared. It was revealed that there is no significant difference in the Harris score between the
two groups 6 months after the operation. The three-point locating method is faster and more accurate than the routine
locating method.
6.
• Manish RShahet al in 2023 Conducted a study on Surgical and Functional Outcomes of the Results of
Conventional Two-Screw Proximal Femoral Nail (PFN) Versus Helical-Blade Anti-rotation Proximal Femoral
Nail (PFNA2)The union time was nearly the same in the majority of the patients, with an early union seen
with the use of PFNA2 nails. The overall modified Harris hip score (HHS) at the final follow-up was nearly
the same with slightly better results with the use of PFNA2. Conclusions PFNA2 is the implant of choice in
elderly patients with osteoporotic bone. It has less operative time, which is required in such patients with
medical comorbidities; hence, it has marginal superiority over PFN. Short-nail design results in less operative
time and less blood loss.
7.
Research question
• Whichimplant (twin screw derotation type or single helical
blade type cephalomedullary nail ) gives better results in
terms of fracture union and less complications in the
treatment of Intertrochanteric femur fractures?
8.
Aims and objectives
•AIM
• To study and compare the results of surgical management of Inter-trochanteric femoral fractures treated by
twin screw derotation type or single helical blade type cephalomedullary nail
• OBJECTIVES
• To compare and find out the ease of use of implant and time taken in fracture union in terms of radiological
outcome and functional restoration.
• To compare and study the complications associated with the individual implant and their management.
9.
Sample size
• Astudy will be conducted on 58 adult patients (both male and female above the age of 50 years)
with Intertrochanteric femoral fractures attending the Outpatient Department/Emergency of the
Department of Orthopedics.
• 29 Patients each will be randomly (by chit method) selected as per inclusion and exclusion criteria
by using odd/even technique for twin screw derotation type or single helical blade type
cephalomedullary nail fixation.
10.
• The samplesize was calculated by using a formula of simple random
sampling for finite population.
• Sample size (n)=2 σ2
(Z α + Z β)2
• d2
• Where: - (All values are taken from blood loss table, in a comparative study
between PFN and PFN-A2 – done by Mandal et al.)
• σ=12.2,
• d= 82.67-73.33 = 9.27,
• Z α=1.96 area of standard normal variate at 95 % confidence interval,
• Z β= 0.84area of standard normal variate at 80 % power
• n= 2 X (12.2)2 (1.96+0.84)2 = 2 X (148.84) (7.84) = 2333.8112 = 27.1585
• (9.27)2 (85.9329) 85.9329
• n = 29 (assuming a non-response rate of 05%)
11.
• INCLUSION CRITERIA-
•1)Age->18years
• 2)Stable and unstable Intertrochanteric fractures (Reverse oblique fractures
and I.T. fractures with posteromedial communition)
• 3) patients who give consent
• EXCLUSION CRITERIA-
• 1)Age less than 18 years
• 2)Segmental fractures
• 3)Fractures more than 1 month old
• 4)Ipsilateral fracture shaft femur with intertrochanteric fracture
• 5)Pathological fractures
• 6)Peri-prosthetic fractures
• 7) polytraumatic patients
• 8) Contralateral limb pathology
12.
Study type
• Aprospective Randomized controlled study to find out the ease of use of implant
and time taken in fracture union in terms of radiological outcome and functional
restoration and to study the complication associated with individual implant.
13.
PREOPERATIVE EVALUATION
• X-Rayof the fractured hip is taken along with the thigh and length and size of implant is determined
depending upon the degree of comminution of fracture, medullary cavity, anterior femoral bow and quality of
bone. Preoperative counseling of the patient and his relatives regarding the method of treatment and
prognosis will be done and consent for operation will be taken. Patient will be immunized against Tetanus.
• Local preparation of the part will be done by shaving and appropriate broad-spectrum antibiotic will be given
a night before the operation and continued thereafter intra and postoperatively.
14.
• Postoperative protocol
•Intravenous antibiotics will be continued. The suction drain will be removed after 48 hours along with 1st
wound check-up. Dynamic quadriceps exercises will be started from day 3. Gait training with partial weight
bearing will be started from day 7 depending on the patient’s compliance. The sutures will be removed on the
10th-12th postoperative day.
• Follow-up and Result evaluation
• All patients will be advised regular follow-up at 3 weekly intervals, till the 12th postoperative week. Further
follow-up will be advised for the patients who will show complications associated with twin screw derotation
type or single helical blade type cephalomedullary nail . Weight-bearing will be gradually increased as per the
radiological evaluation of the fractured site. The hip scoring will be done as per the following:
15.
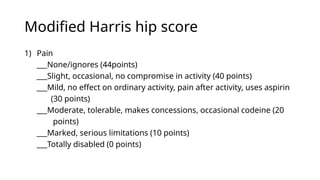
Modified Harris hipscore
1) Pain
___None/ignores (44points)
___Slight, occasional, no compromise in activity (40 points)
___Mild, no effect on ordinary activity, pain after activity, uses aspirin
(30 points)
___Moderate, tolerable, makes concessions, occasional codeine (20
points)
___Marked, serious limitations (10 points)
___Totally disabled (0 points)
16.
2) Function: Gait
Limp
None(11l points)
Slight (8 points)
Moderate (5 points)
Severe (0 points)
Unable to walk (0 points)
Support
None (11 points)
Cane. Lorig walks (7 points)
Cane, full time (5 points)
Crutch (4 points)
2 canes (2 points)
2 crutches (1 points)
Unable to walk ( points).
Distance Walked
Unlimited (1l points)
6 blocks (8 points)
2-3 blocks (5 points)
Indoors only (2 points)
Bed and chair (0 points)
17.
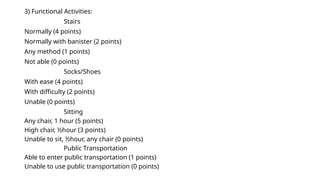
3) Functional Activities:
Stairs
Normally(4 points)
Normally with banister (2 points)
Any method (1 points)
Not able (0 points)
Socks/Shoes
With ease (4 points)
With difficulty (2 points)
Unable (0 points)
Sitting
Any chair, 1 hour (5 points)
High chair, ½hour (3 points)
Unable to sit, ½hour, any chair (0 points)
Public Transportation
Able to enter public transportation (1 points)
Unable to use public transportation (0 points)
18.
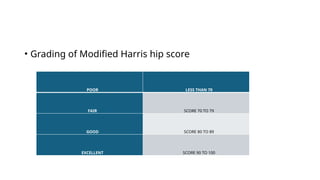
• Grading ofModified Harris hip score
POOR LESS THAN 70
FAIR SCORE 70 TO 79
GOOD SCORE 80 TO 89
EXCELLENT SCORE 90 TO 100
19.
STATISTICAL ANALYSIS
• Thedata will be captured on the physical proforma and a master chart will be
prepared in the Microsoft Excel. The statistical analysis will carry out using
SPSS 27.0 (IBM, Trialware, USA). Mean will be used as measures of central
tendency for quantitative variables and standard deviation will be used as
measure of variability for quantitative data. Qualitative variable will be
described in frequencies and percentage of total. To compare two
quantitative variables, unpaired and paired t-test will be used whereas one
way ANOVA will be used to compare more than two variables. For qualitative
variables, Chi-square test will be used for comparison between the two
groups. All tests were tested at 5% level of significance and 95% confidence
interval. All statistical tests were performed by taking significance level of α =
0.05. Appropriate tables and graphs will be used to represent the data.
•
22.
Bibliography
• Mallya Set al. Comparison of radiological and functional outcome of unstable intertrochanteric femur
fractures treated using PFN and PFNA-2 in patients with osteoporosis. Eur J Orthop Surg Traumatol. 2019
Jul;29(5):1035-1042.
• Tian RH et al. Comparison of two methods of locating proximal femoral nail anti-rotation in the treatment of
femoral intertrochanteric fractures. J Orthop Surg Res. 2020 Mar 17;15(1):108.
• Shah MR et al. Surgical and Functional Outcomes of the Results of Conventional Two-Screw Proximal
Femoral Nail (PFN) Versus Helical-Blade Anti-rotation Proximal Femoral Nail (PFNA2). Cureus. 2023 Aug
18;15(8):e43698.