Downloaded 182 times
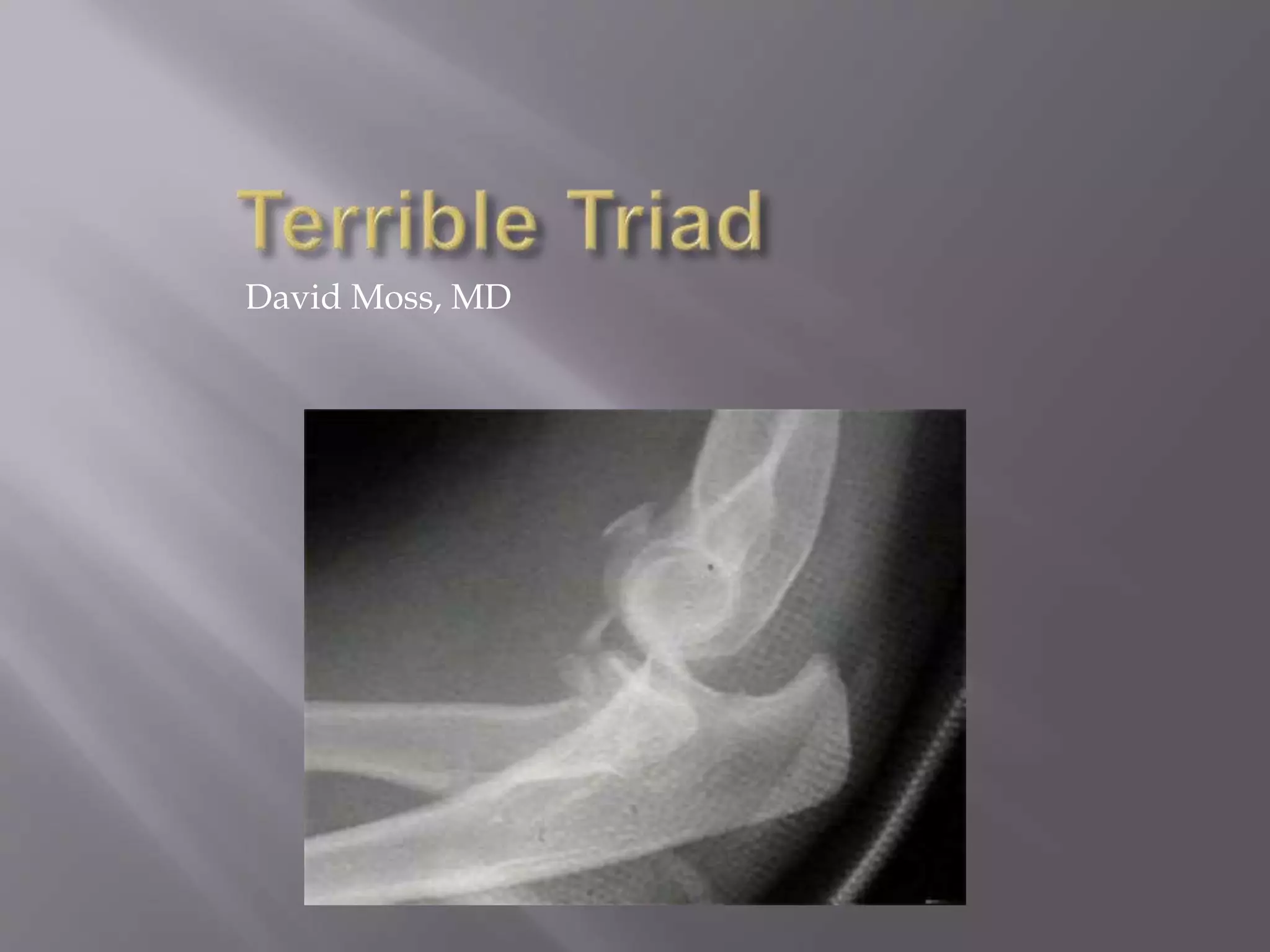
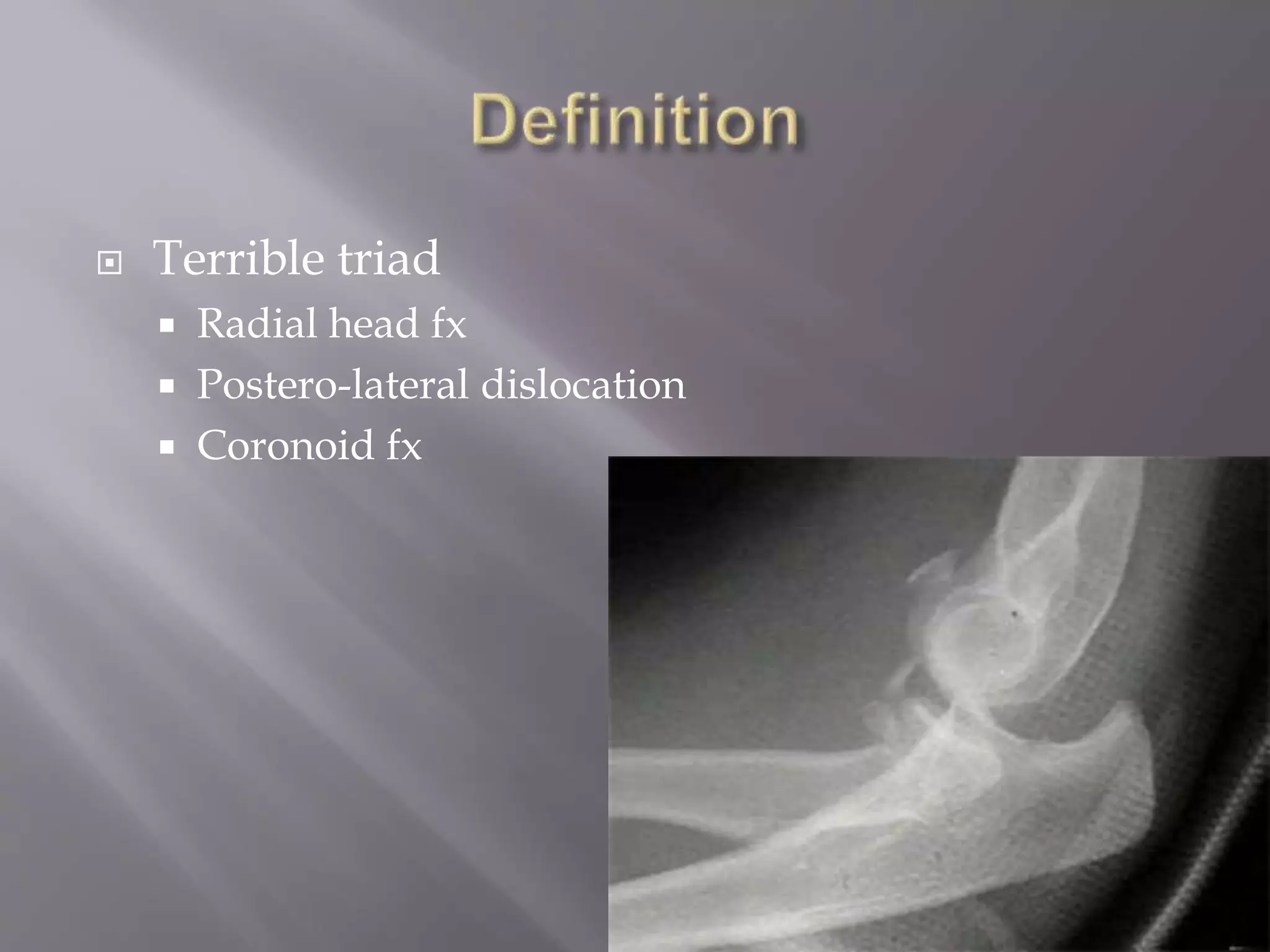
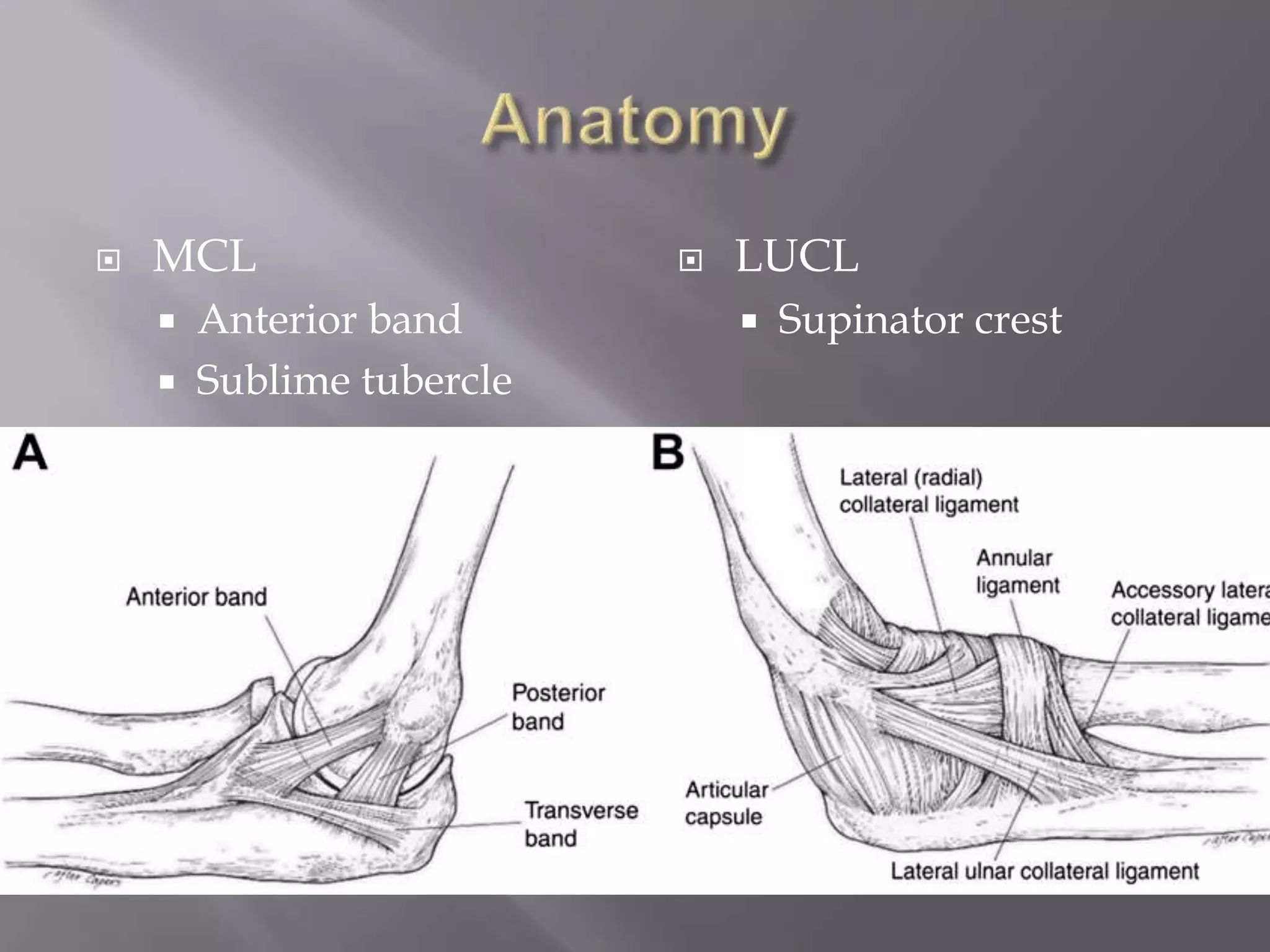
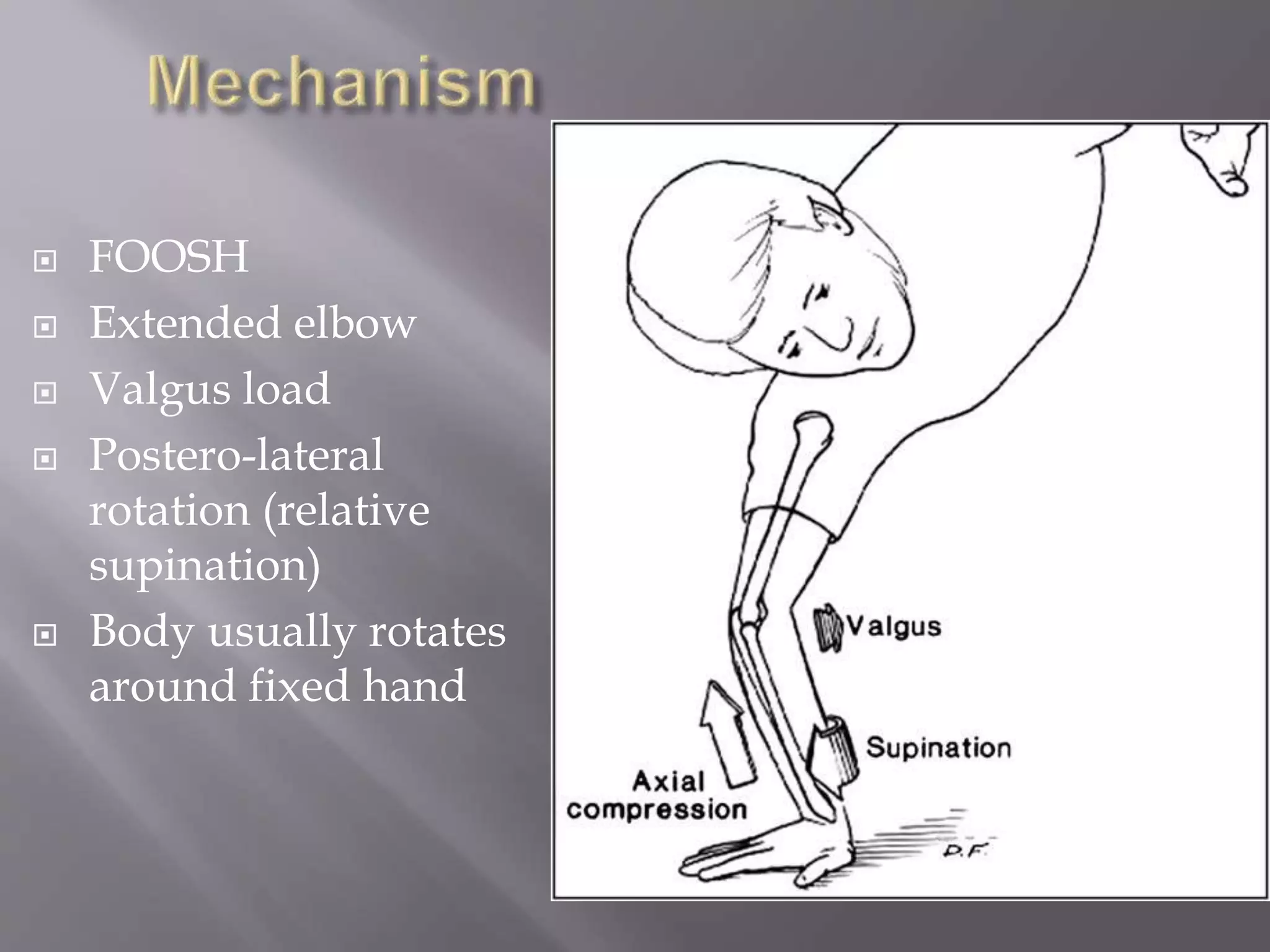
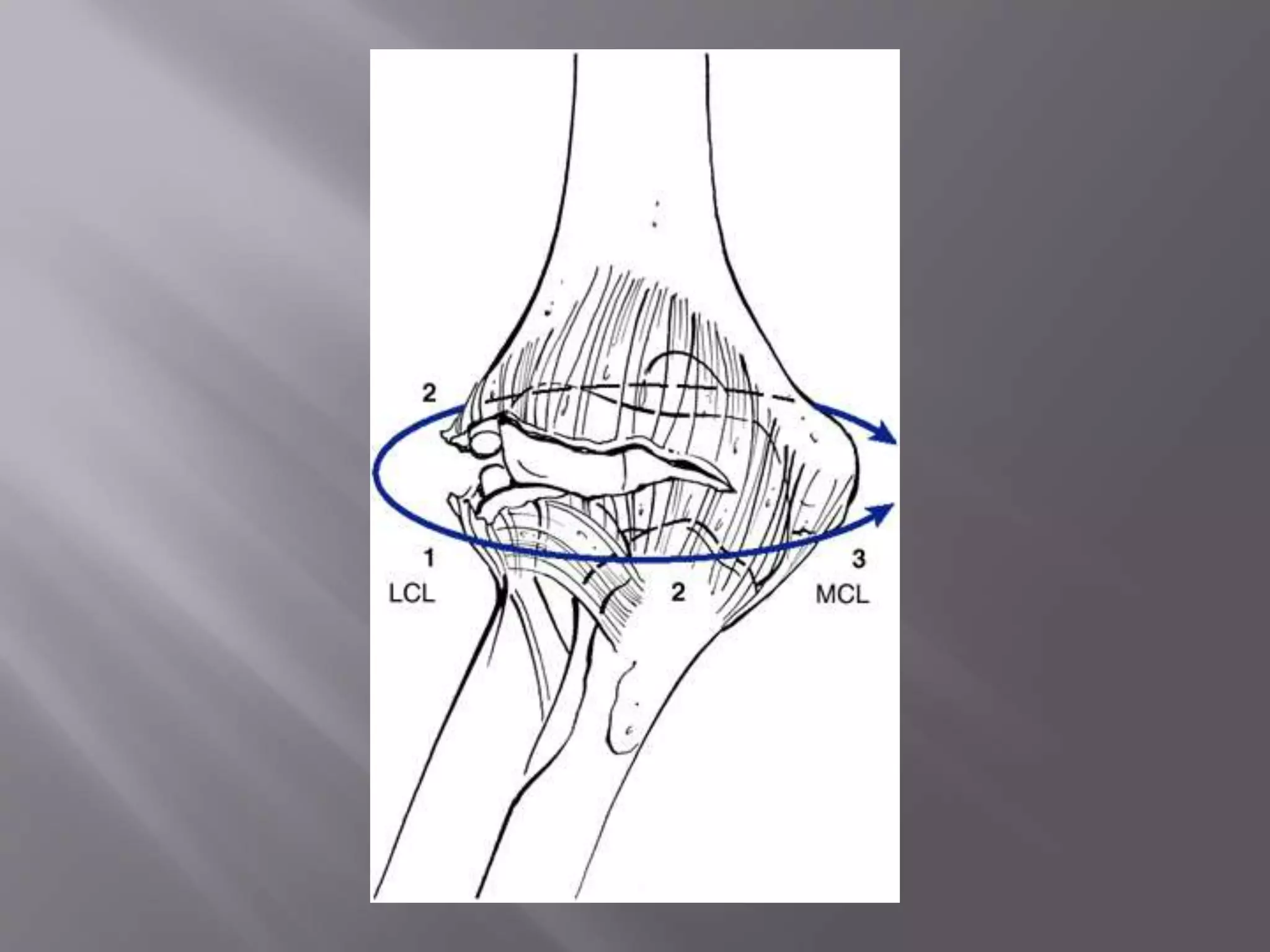
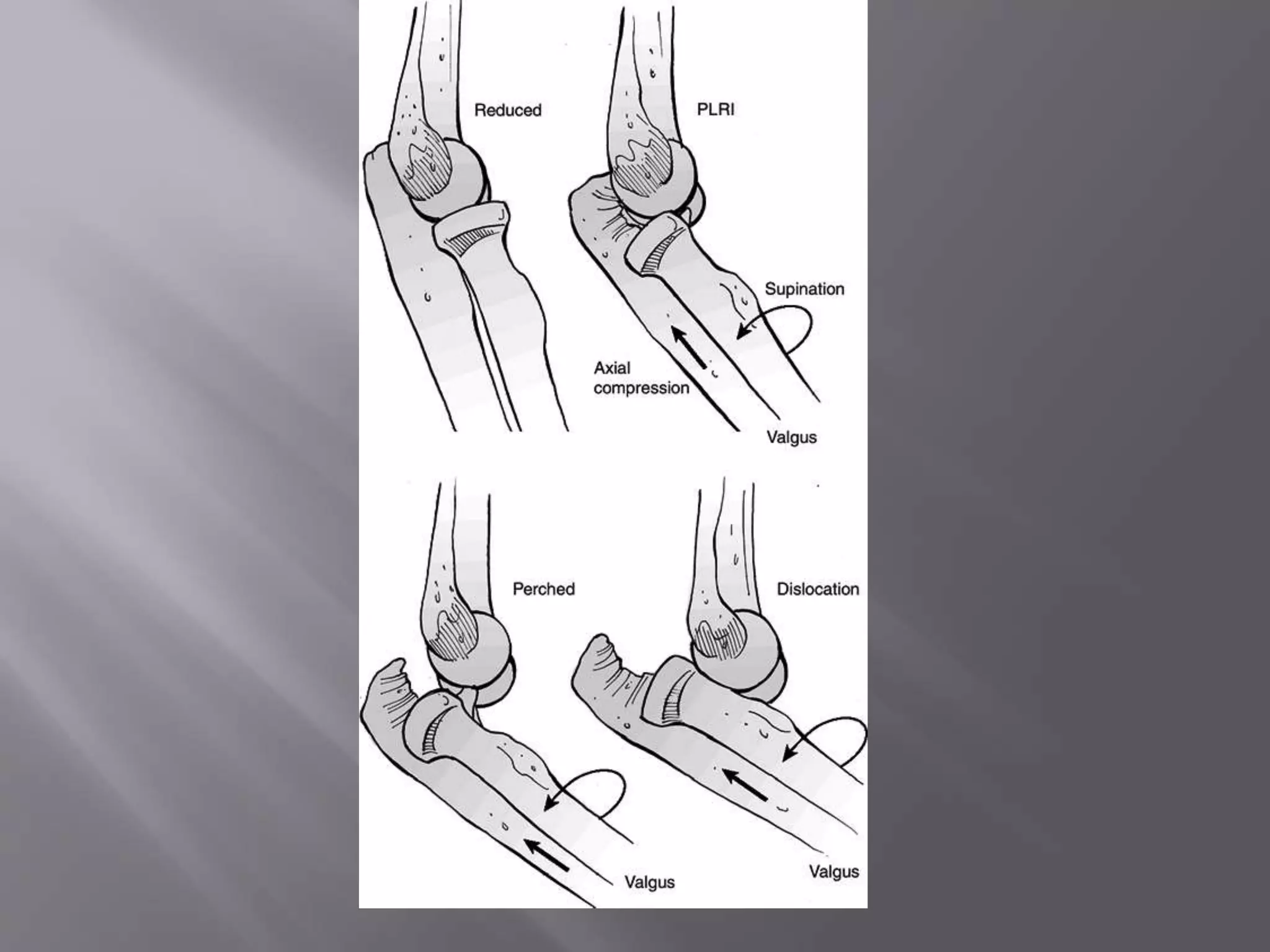
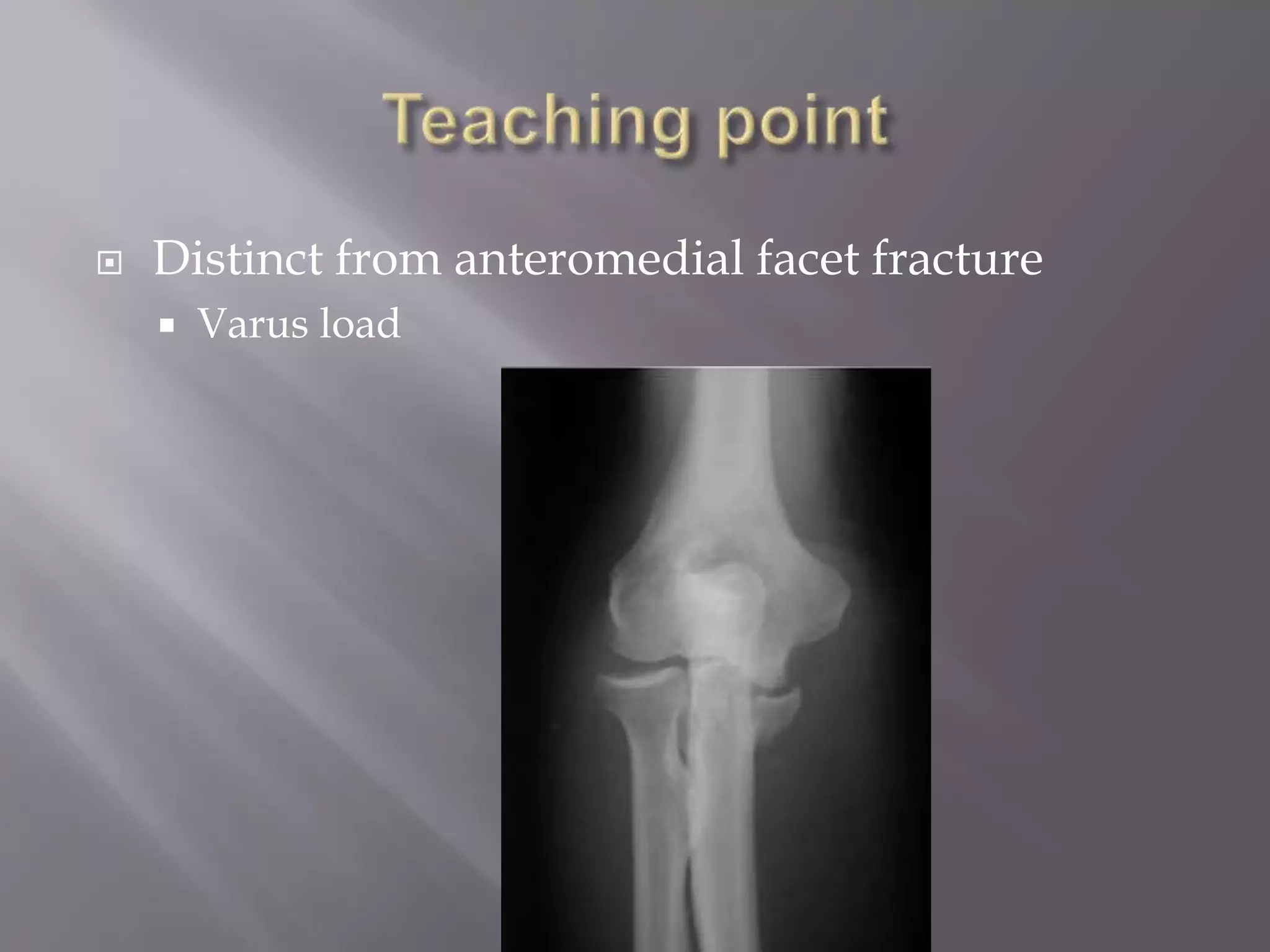
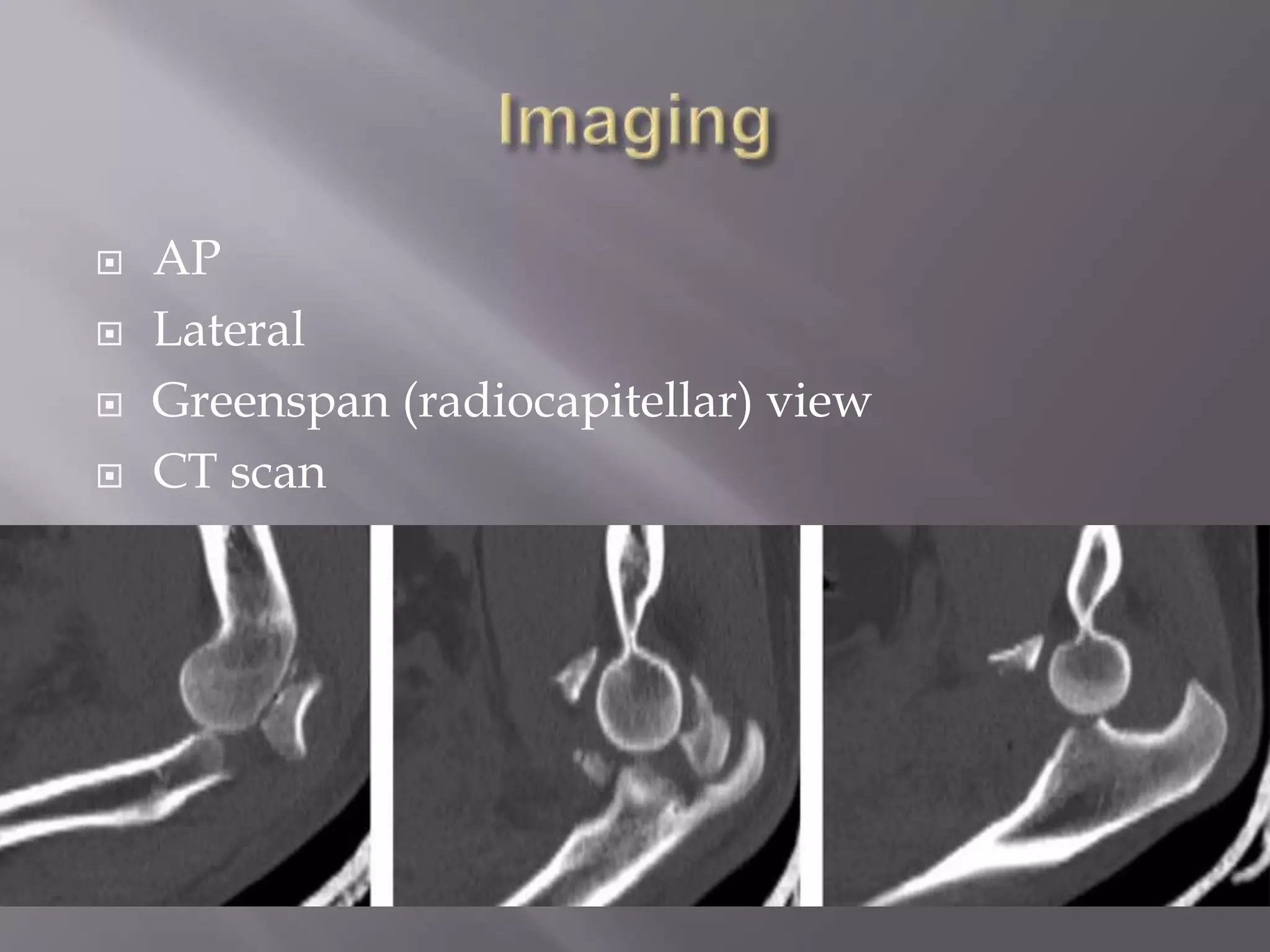


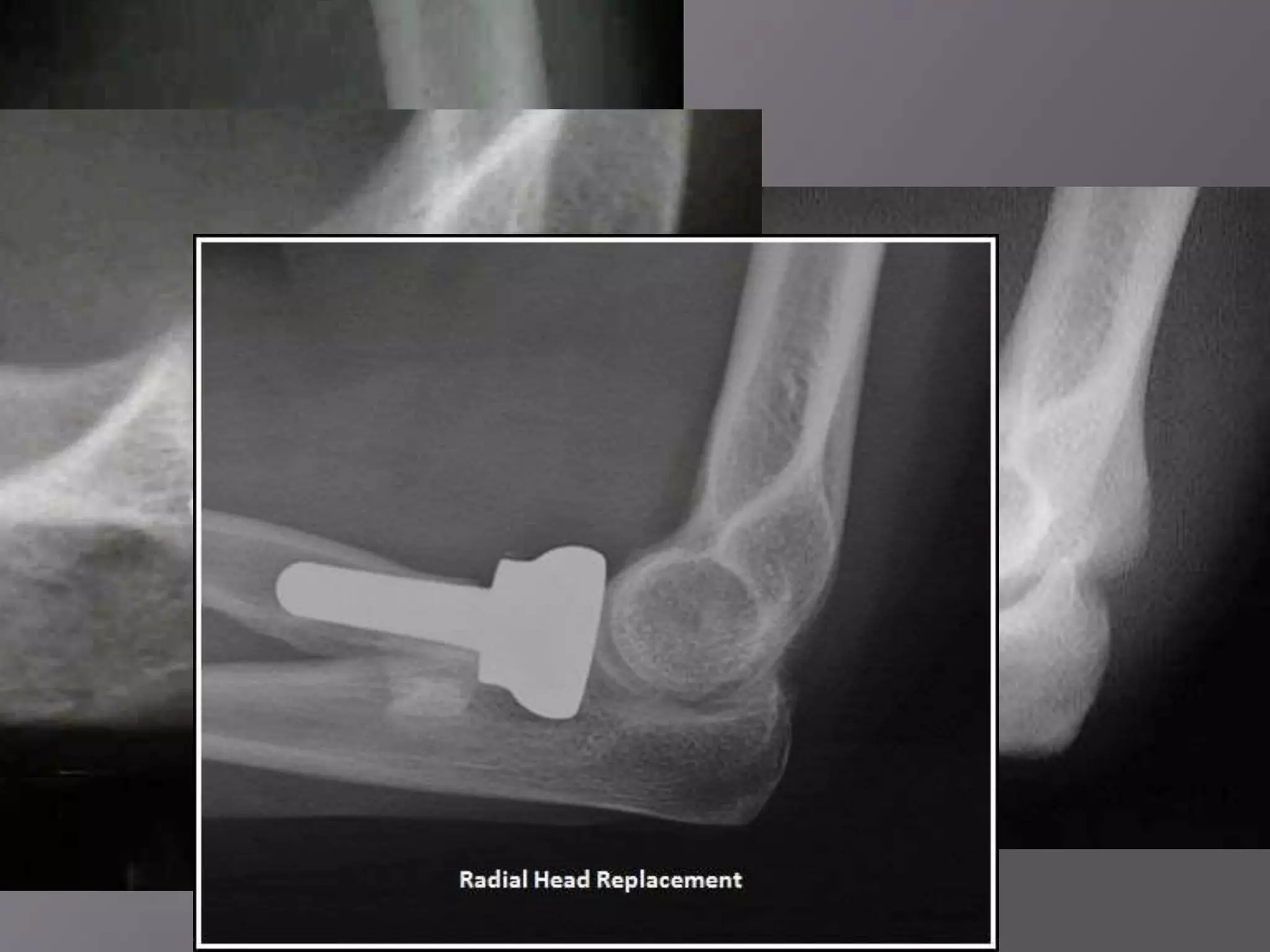





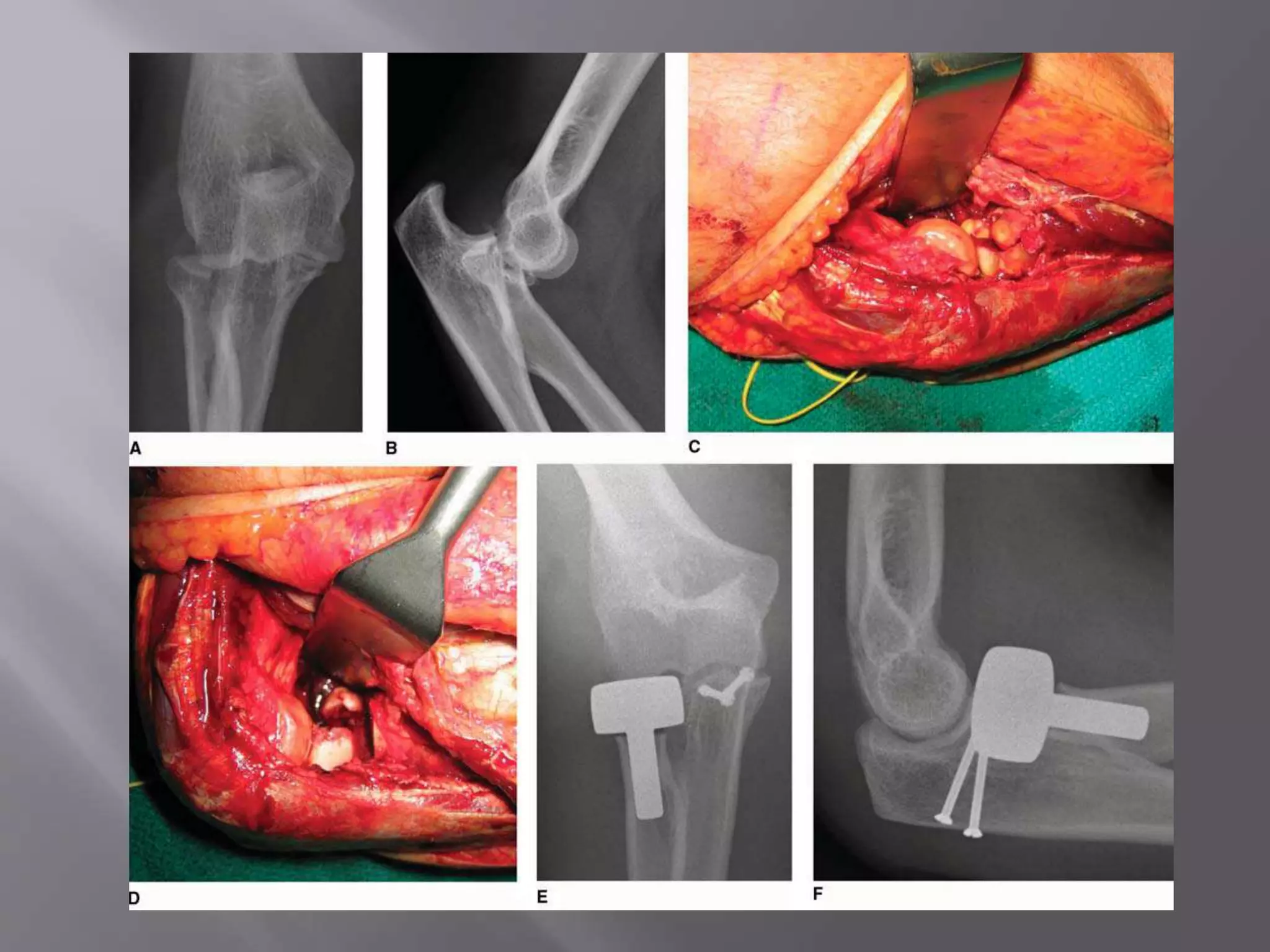

This document discusses the terrible triad injury of the elbow, which involves fractures of the radial head, coronoid process, and posterolateral dislocation. It notes the poor outcomes associated with this injury like stiffness, instability, and hardware failure. The document outlines the relevant anatomy of the medial collateral ligament and lateral uncular collateral ligament. It describes the mechanism of injury, known as the fall on an outstretched hand, and how the ligaments and capsule fail in this injury. Diagnostic imaging and classification of radial head and coronoid fractures are covered. Treatment options including observation, resection, open reduction internal fixation, and replacement are presented. Surgical approaches and techniques are also outlined.


































































![[Sport] mm chronic elbow injury](https://cdn.slidesharecdn.com/ss_thumbnails/sportmmchronicelbowinjury-200208065658-thumbnail.jpg?width=640&height=640&fit=bounds)






































