Downloaded 104 times








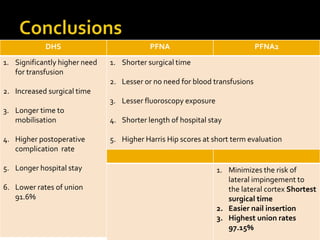


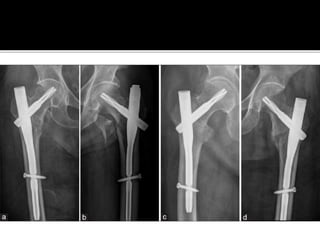

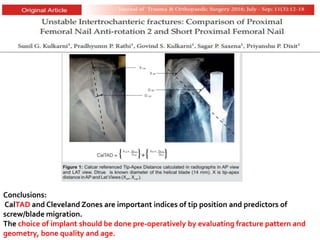
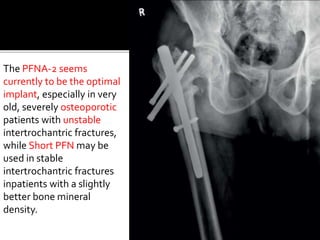
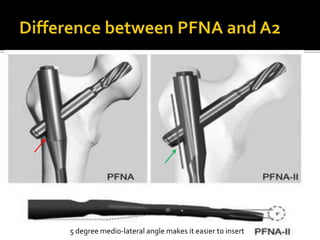
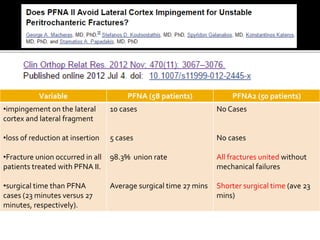

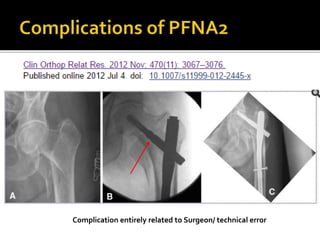

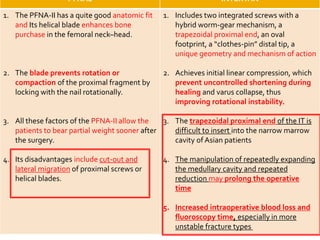


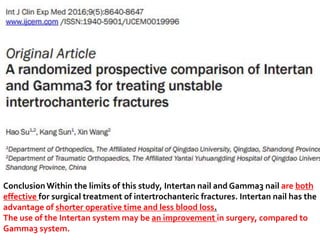
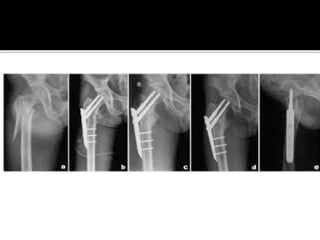







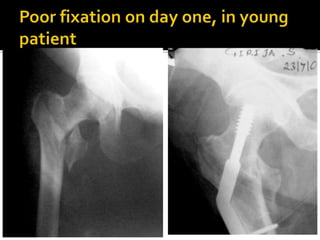





The document discusses advancements in the fixation of intertrochanteric fractures, emphasizing the advantages of intramedullary devices such as the Proximal Femoral Nail Antirotation II (PFNA-2) over traditional methods like Dynamic Hip Screws (DHS). It highlights improved surgical outcomes, including shorter surgical times, lower complication rates, and higher union rates with PFNA-2, while noting the importance of surgical technique in preventing complications. Overall, it concludes that PFNA-2 is a promising choice for unstable intertrochanteric fractures, particularly in elderly patients, although further research is recommended.



















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















