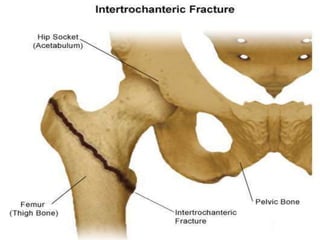
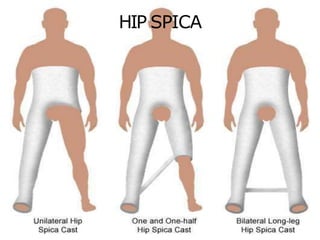
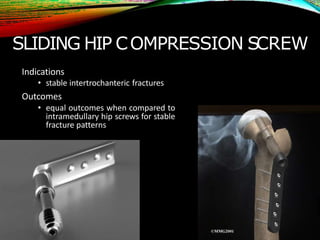
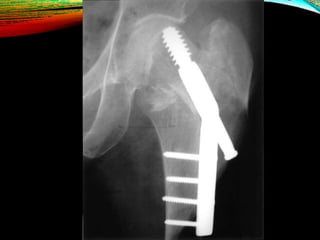
An intertrochanteric fracture occurs between the greater and lesser trochanters of the femur. It commonly affects elderly osteoporotic patients, usually women in their 80s, following a simple fall. X-rays are used to diagnose this extracapsular hip fracture. Treatment involves early internal fixation with devices like the sliding hip screw or intramedullary hip screw to allow early ambulation and prevent complications of non-operative management. Complications can include failure of fixation, malunion, or nonunion if reduction or implant positioning is inadequate.






















![PFFD [proximal femoral focal deficiency]](https://cdn.slidesharecdn.com/ss_thumbnails/pffdproximalfemoralfocaldeficiency-200421181838-thumbnail.jpg?width=640&height=640&fit=bounds)



































![Overview of Fungal Infections[1].ppt pptx](https://cdn.slidesharecdn.com/ss_thumbnails/overviewoffungalinfections1-250811070114-3c4fbad5-thumbnail.jpg?width=640&height=640&fit=bounds)




![Gas gangrene [Autosaved].pptxGas gangrene [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gasgangreneautosaved-250608063811-c85a18a4-thumbnail.jpg?width=640&height=640&fit=bounds)


























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


