Downloaded 197 times
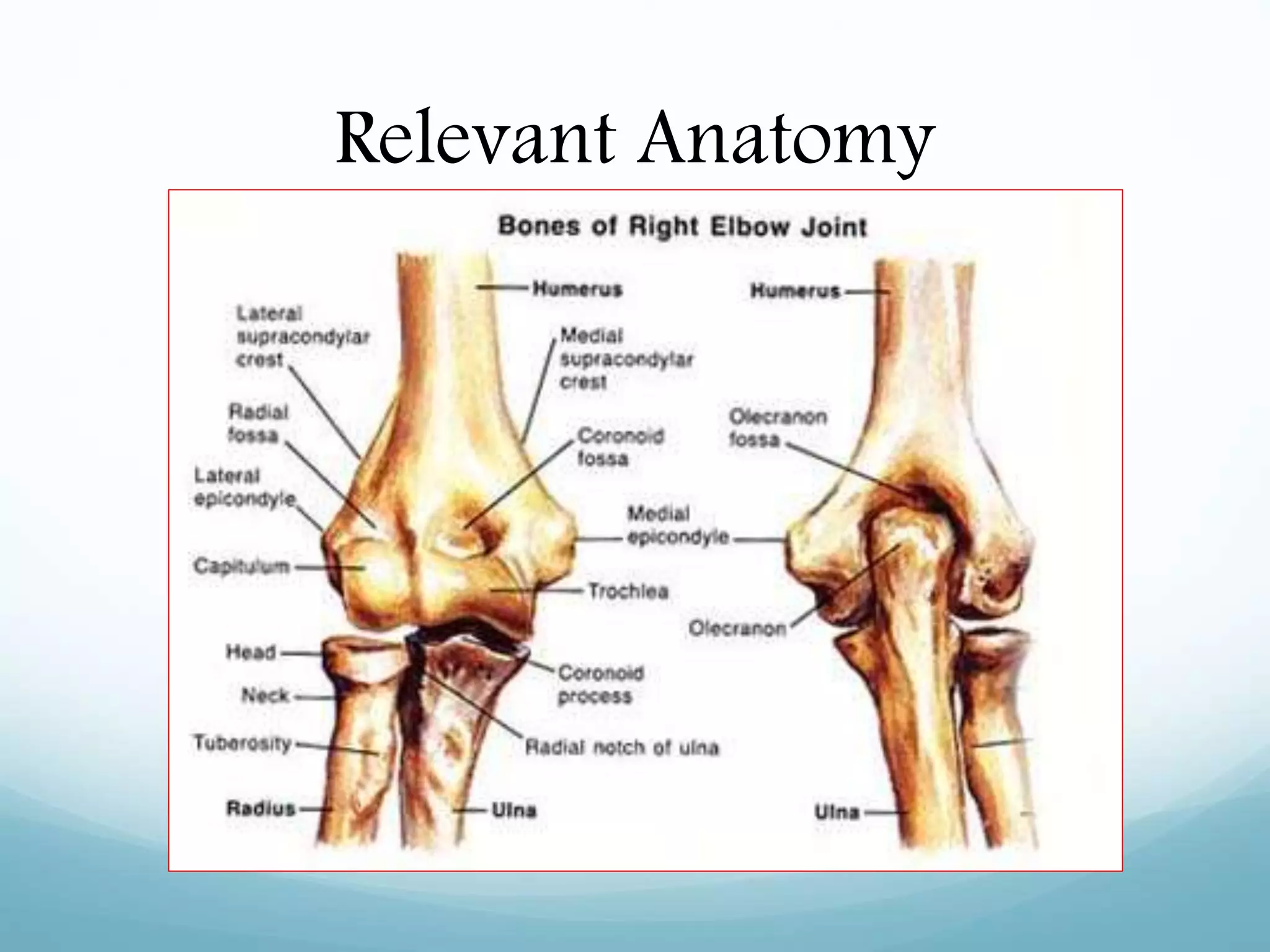
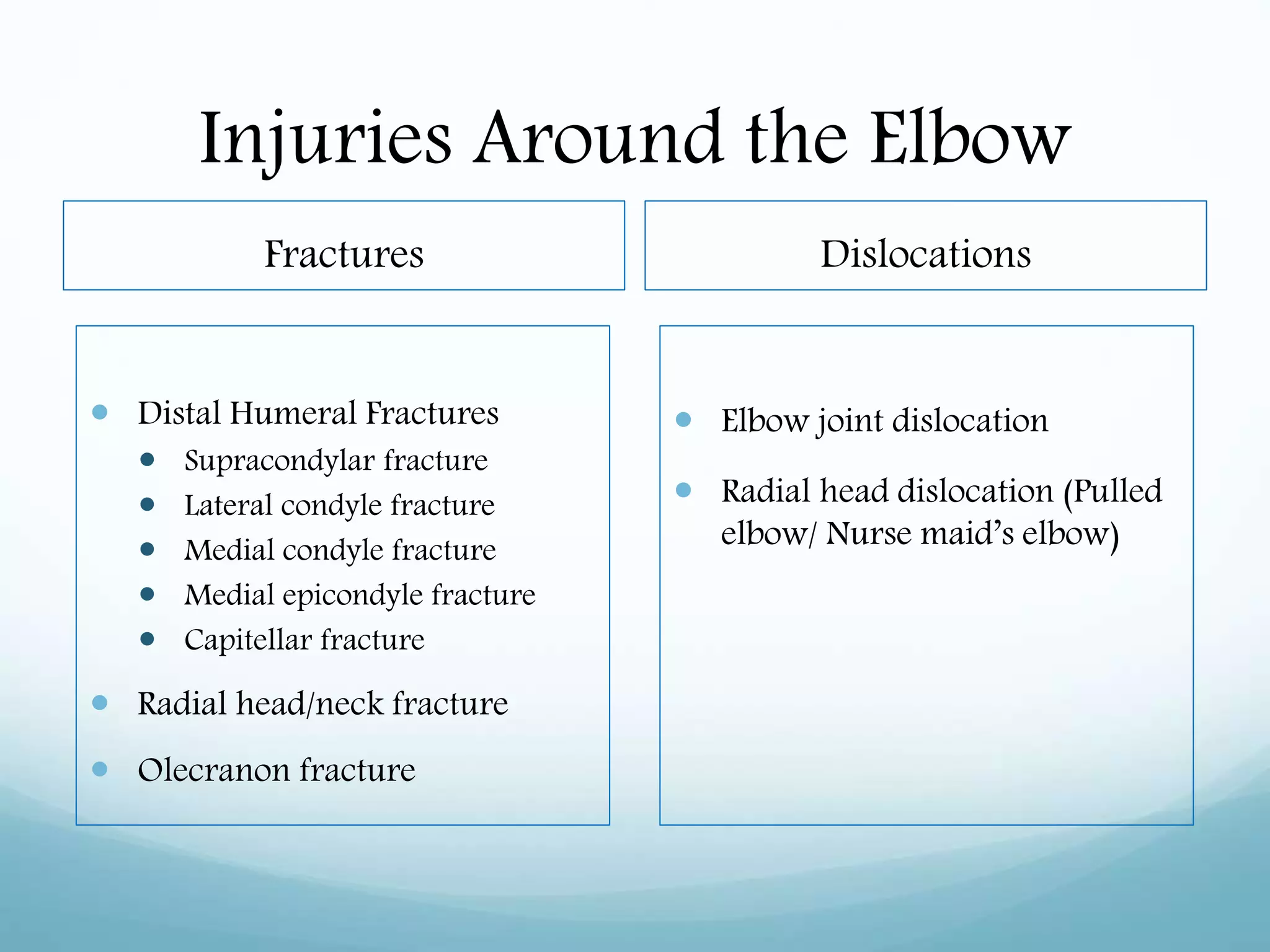
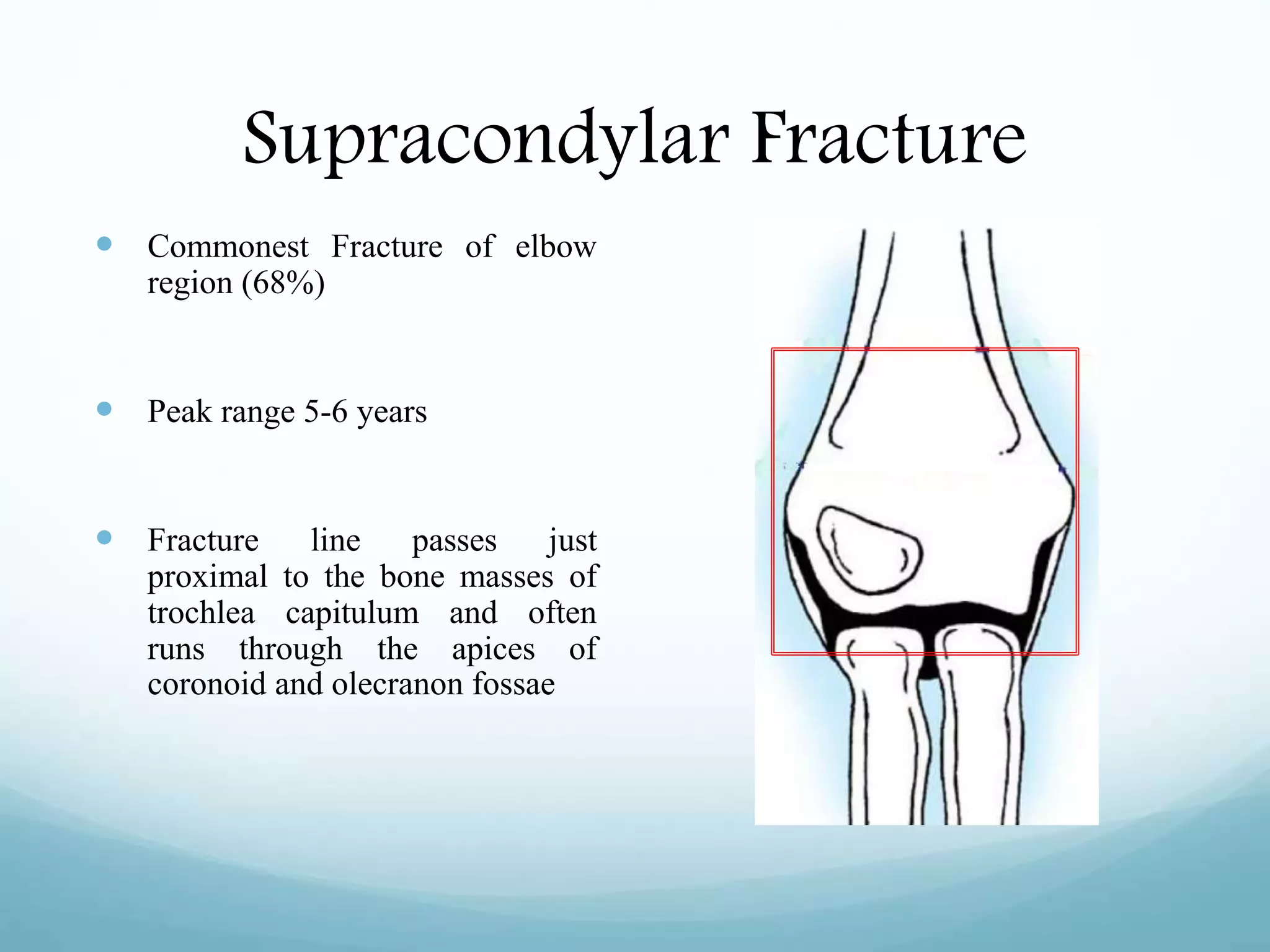
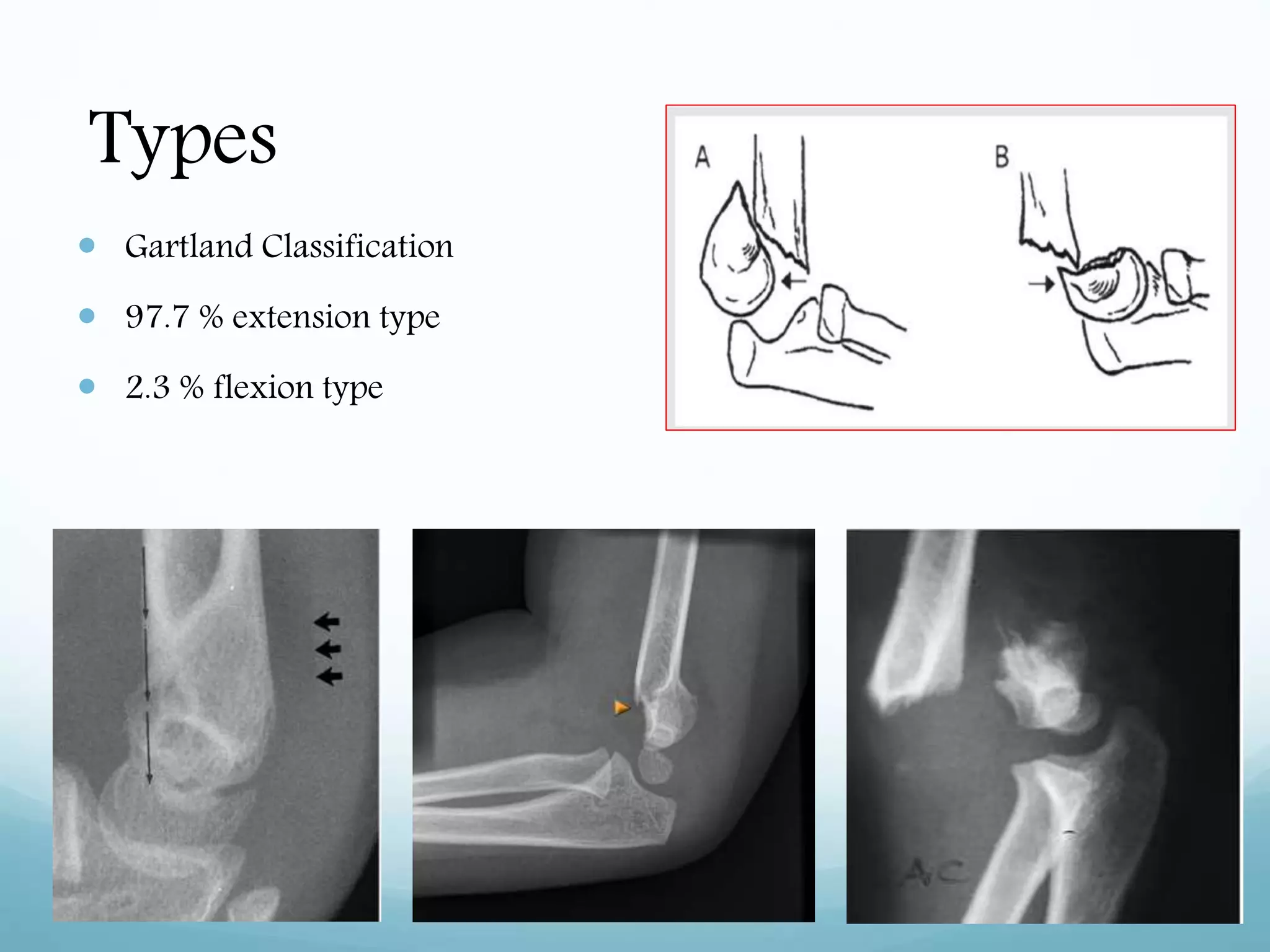
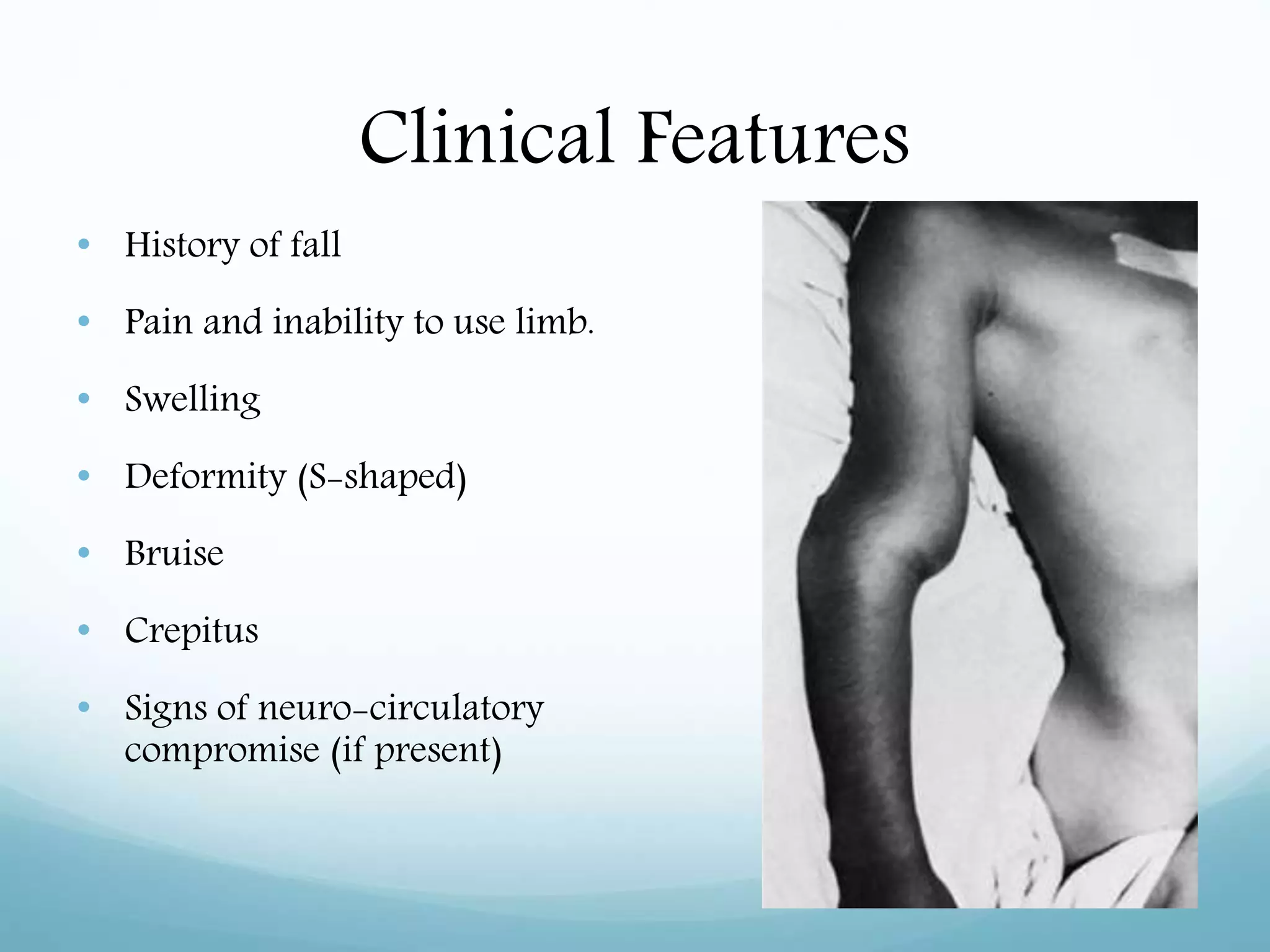

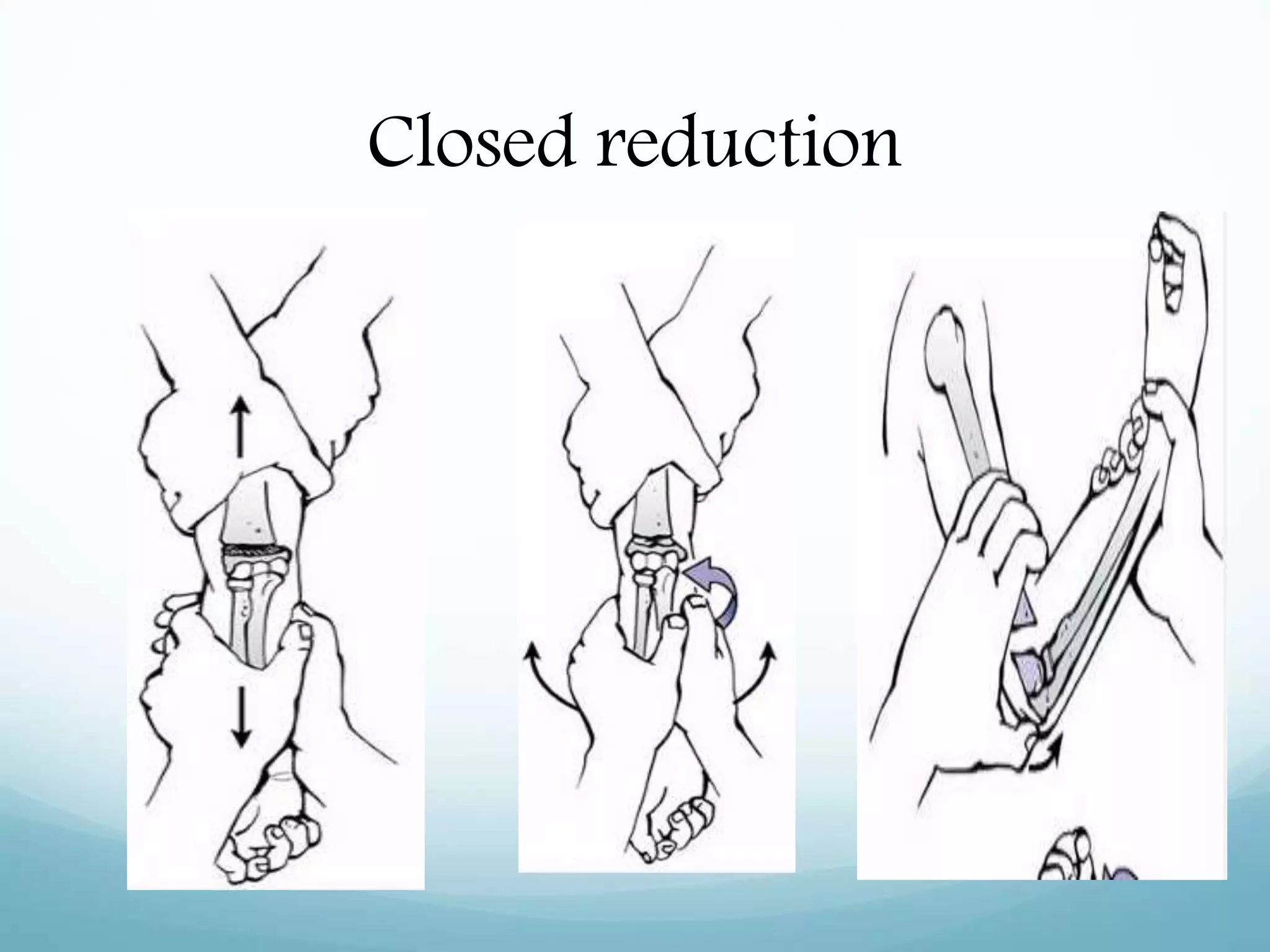









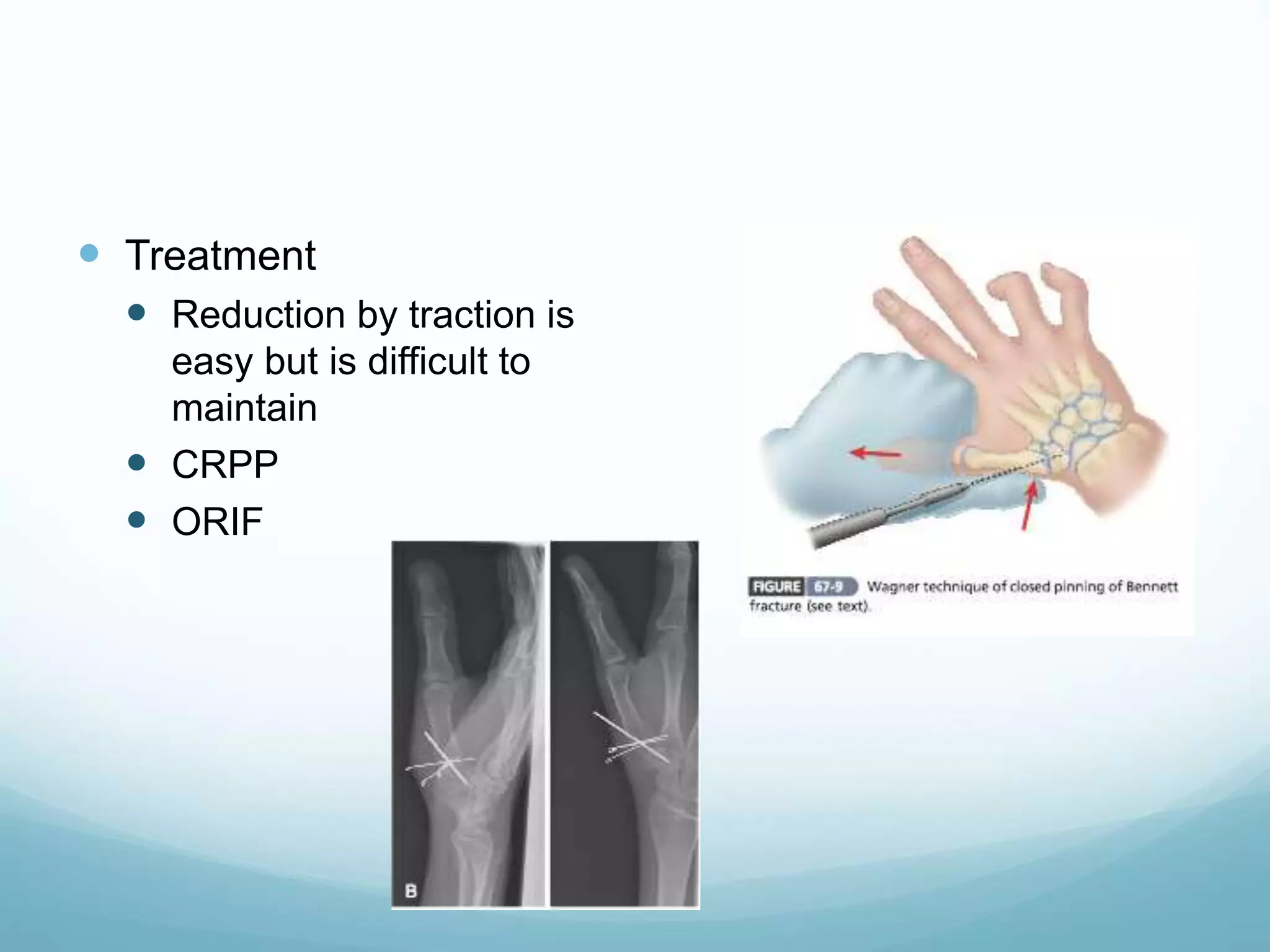
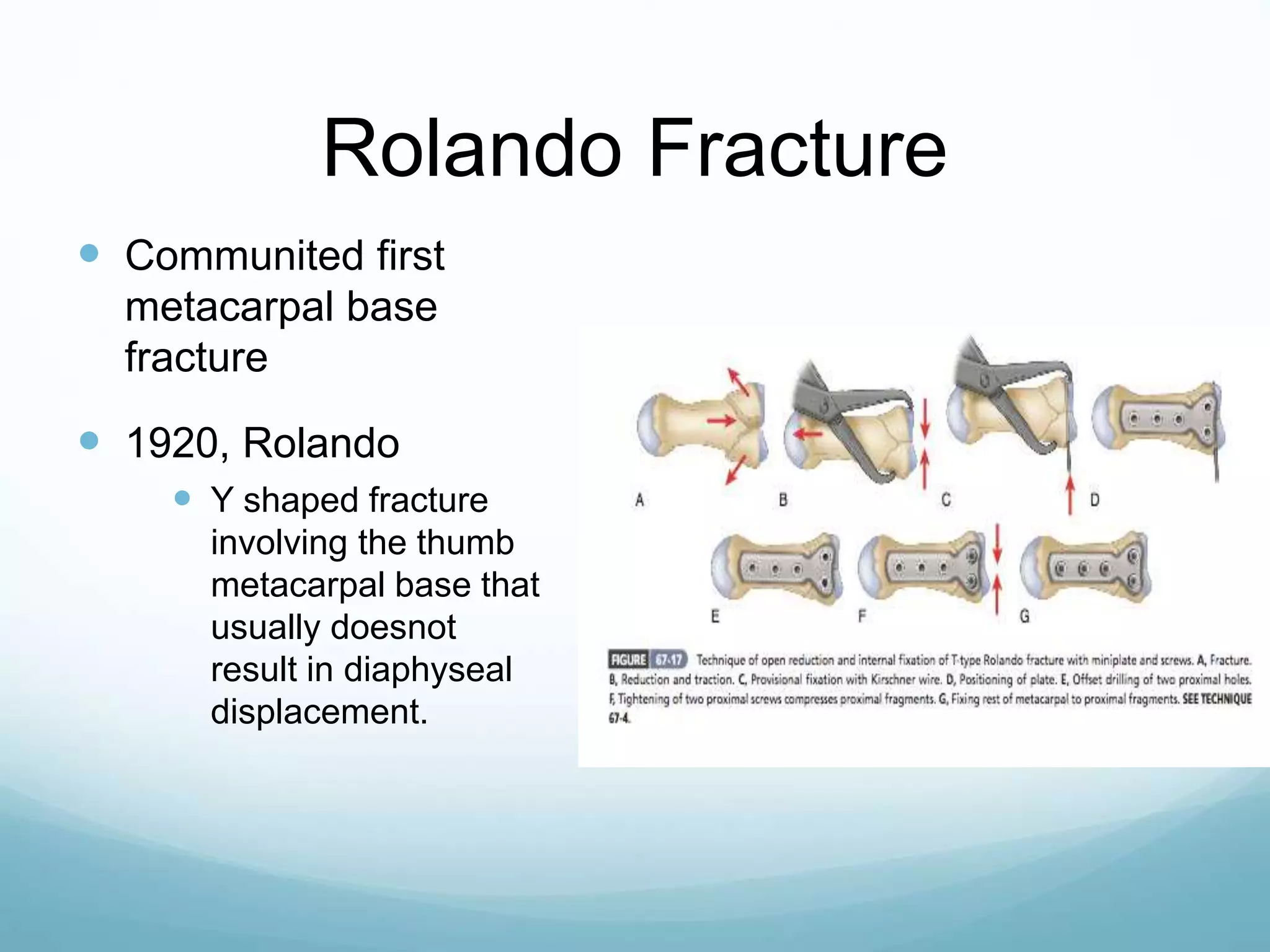
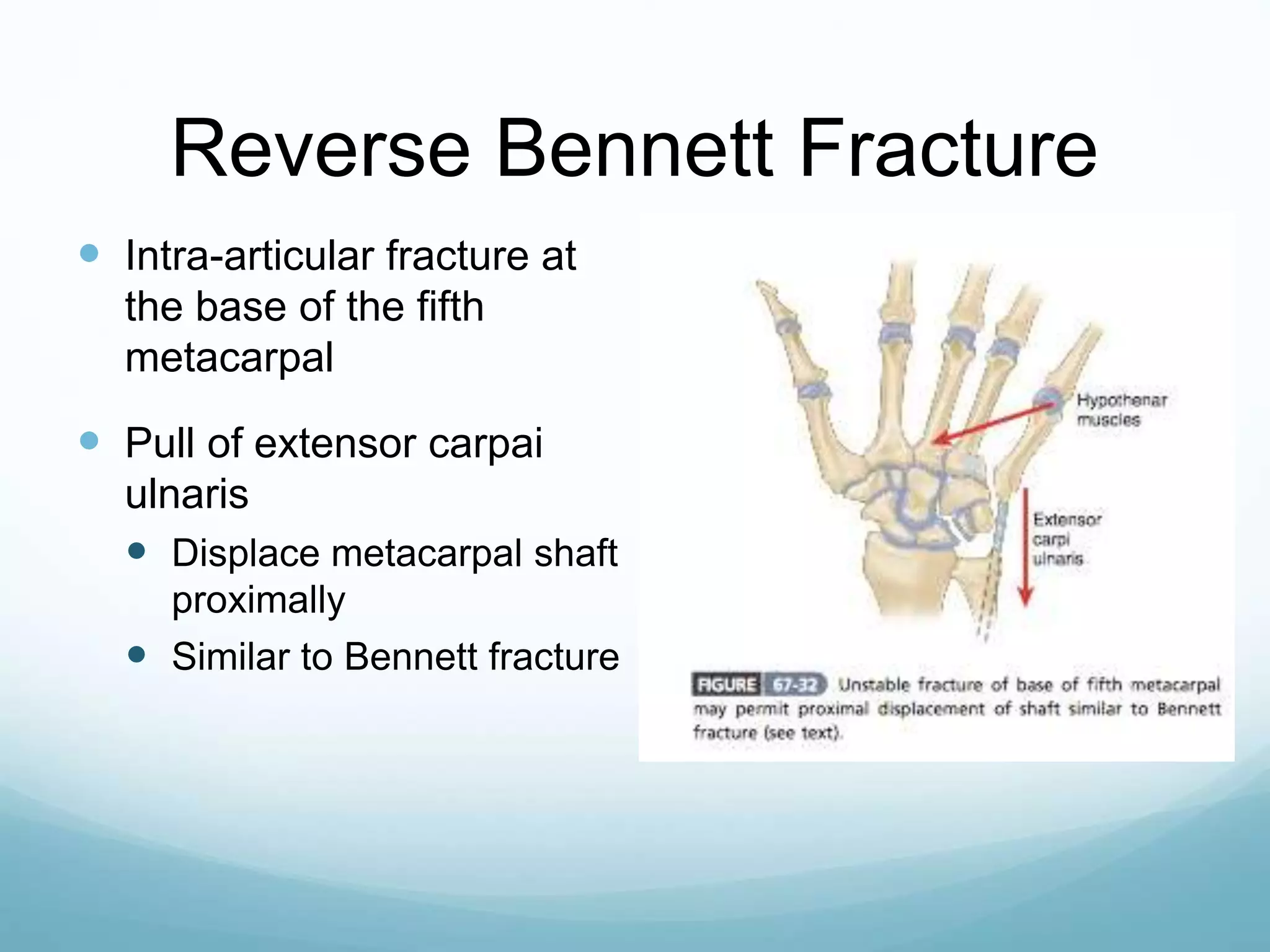
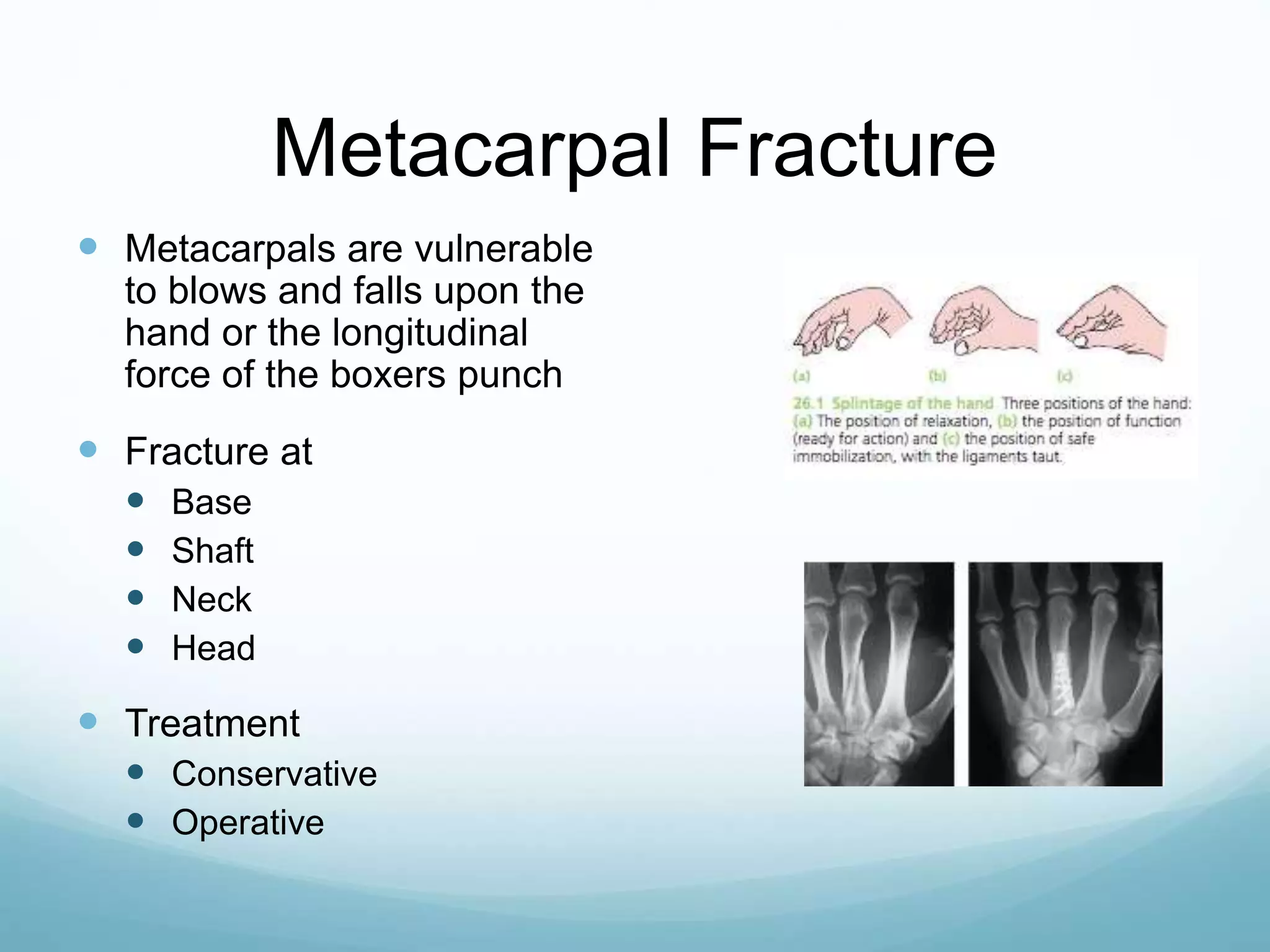


The document discusses various types of elbow and hand fractures, focusing on their anatomy, classifications, clinical features, management, and potential complications. It highlights supracondylar fractures as the most common in children and details treatment options like closed reduction and open reduction with internal fixation. Additionally, it addresses other specific fractures around the elbow and hand, such as lateral condyle and Bennett fractures, along with their treatment procedures.













































































