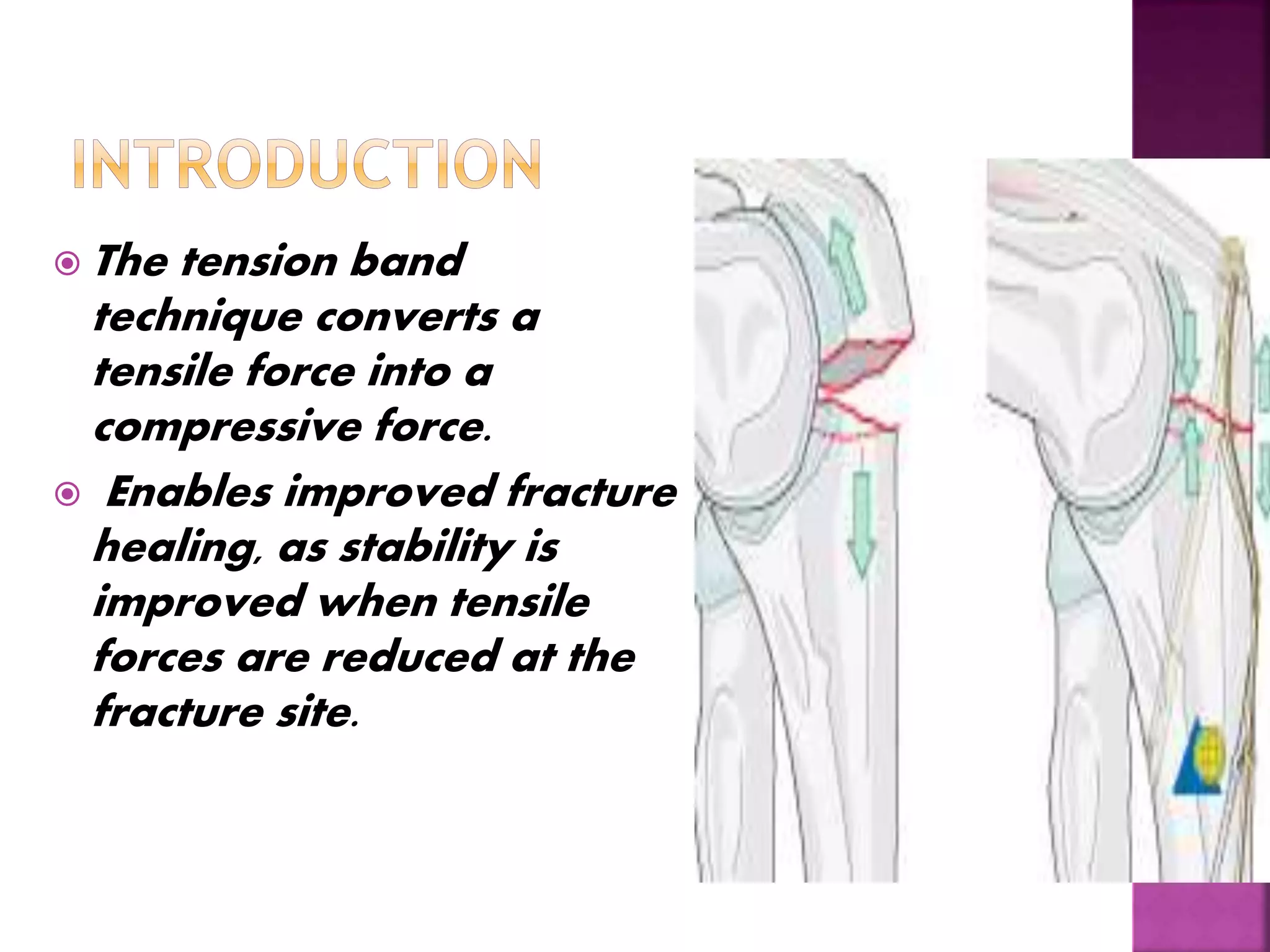
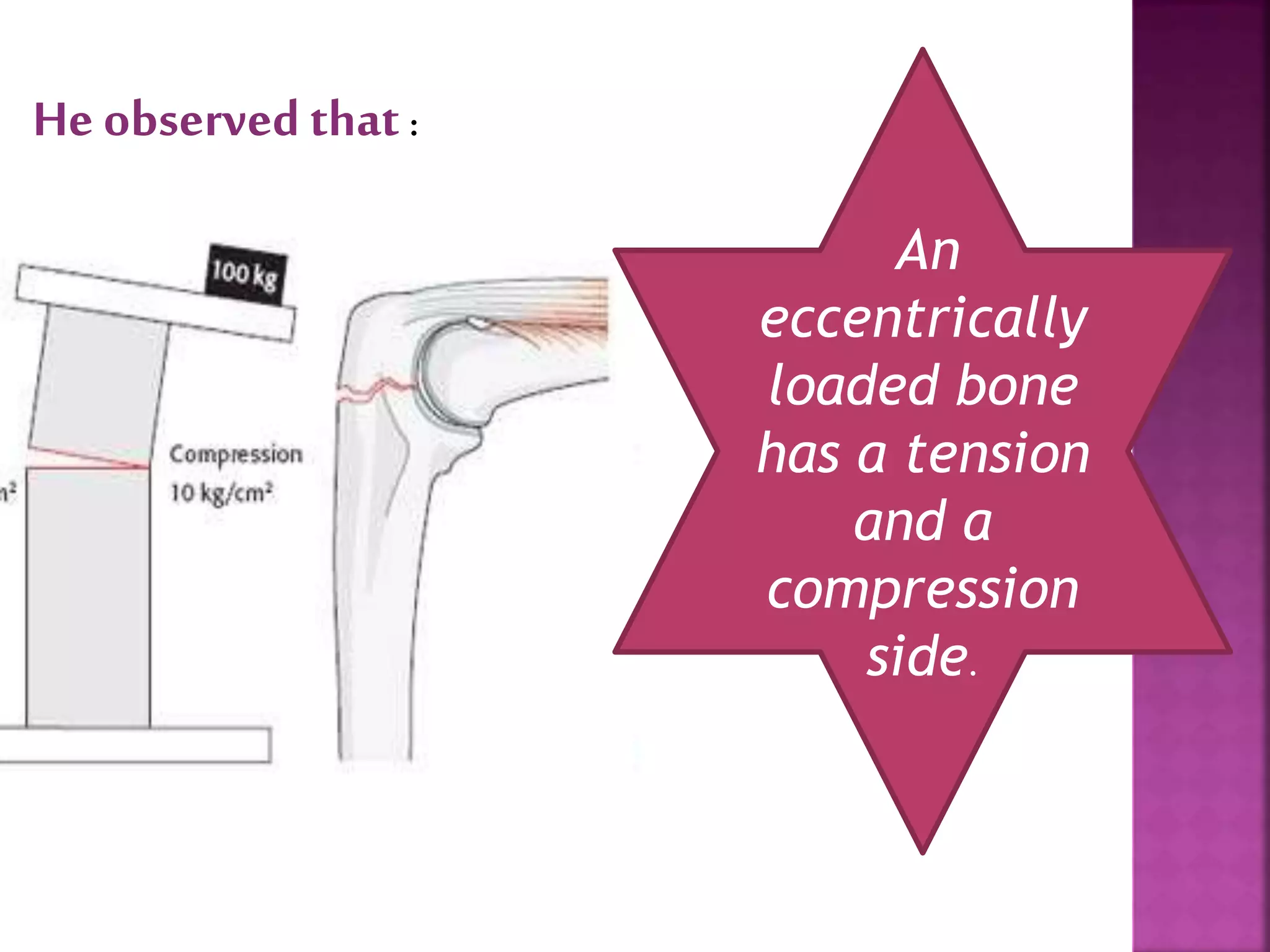
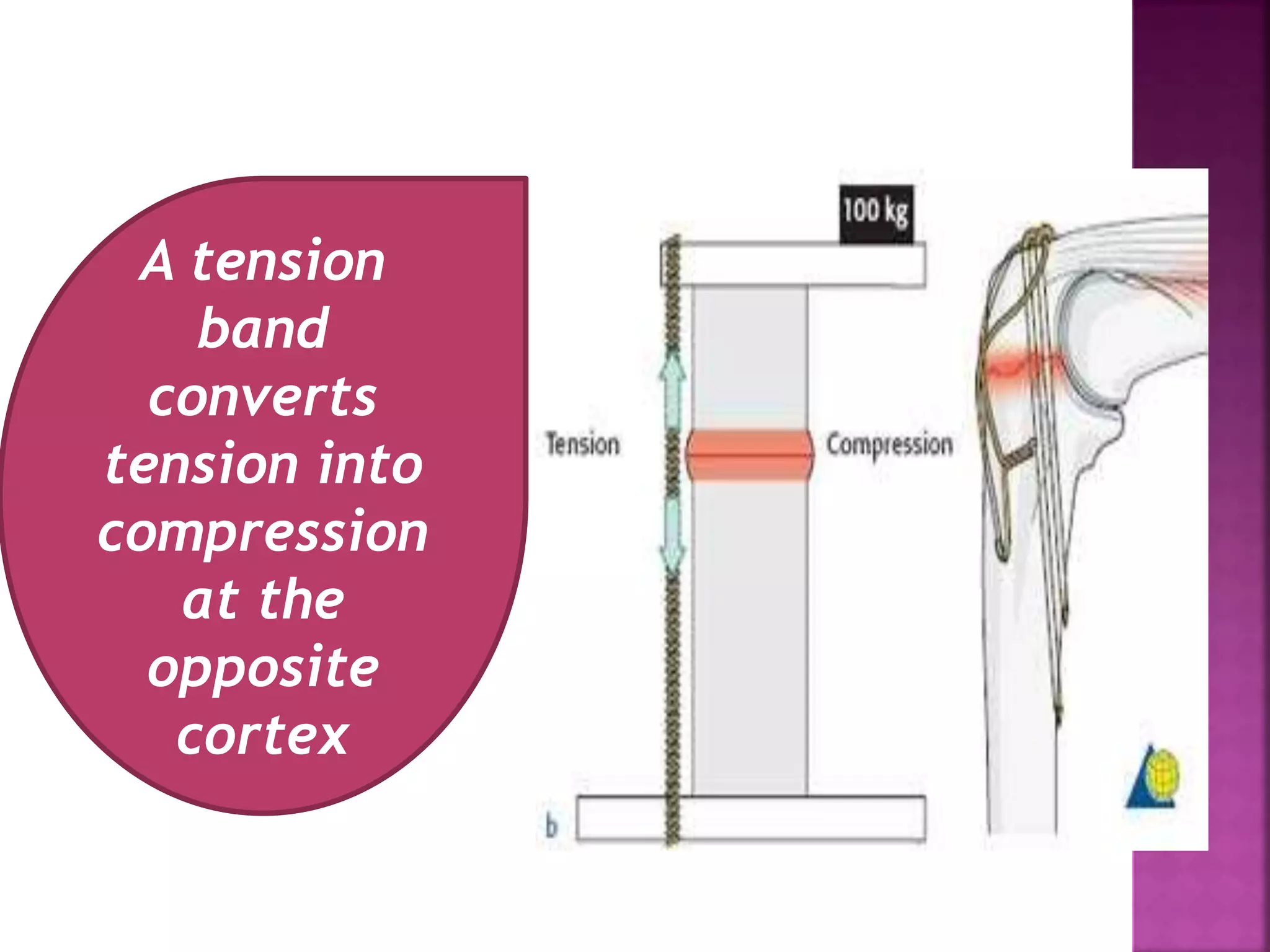
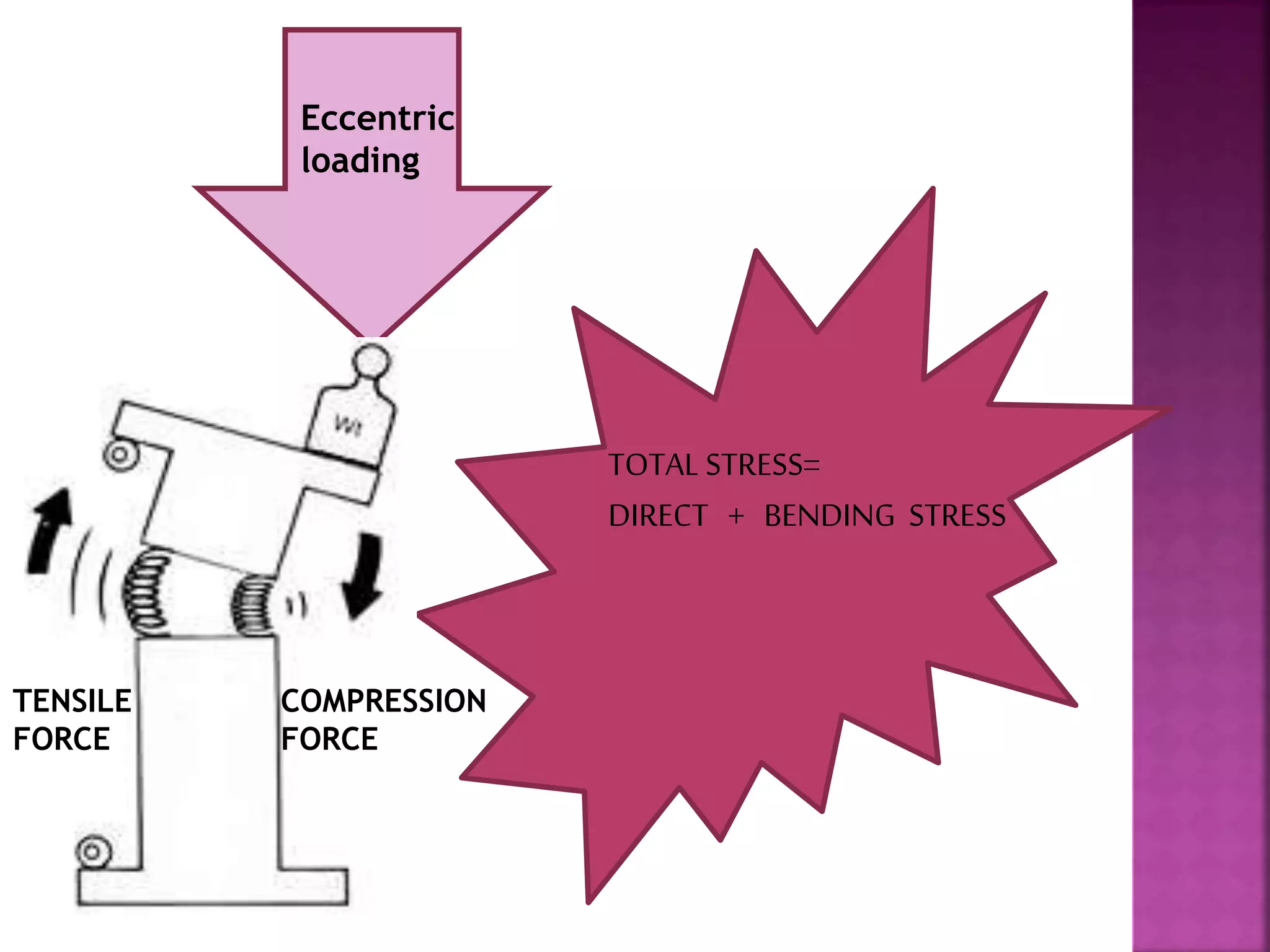
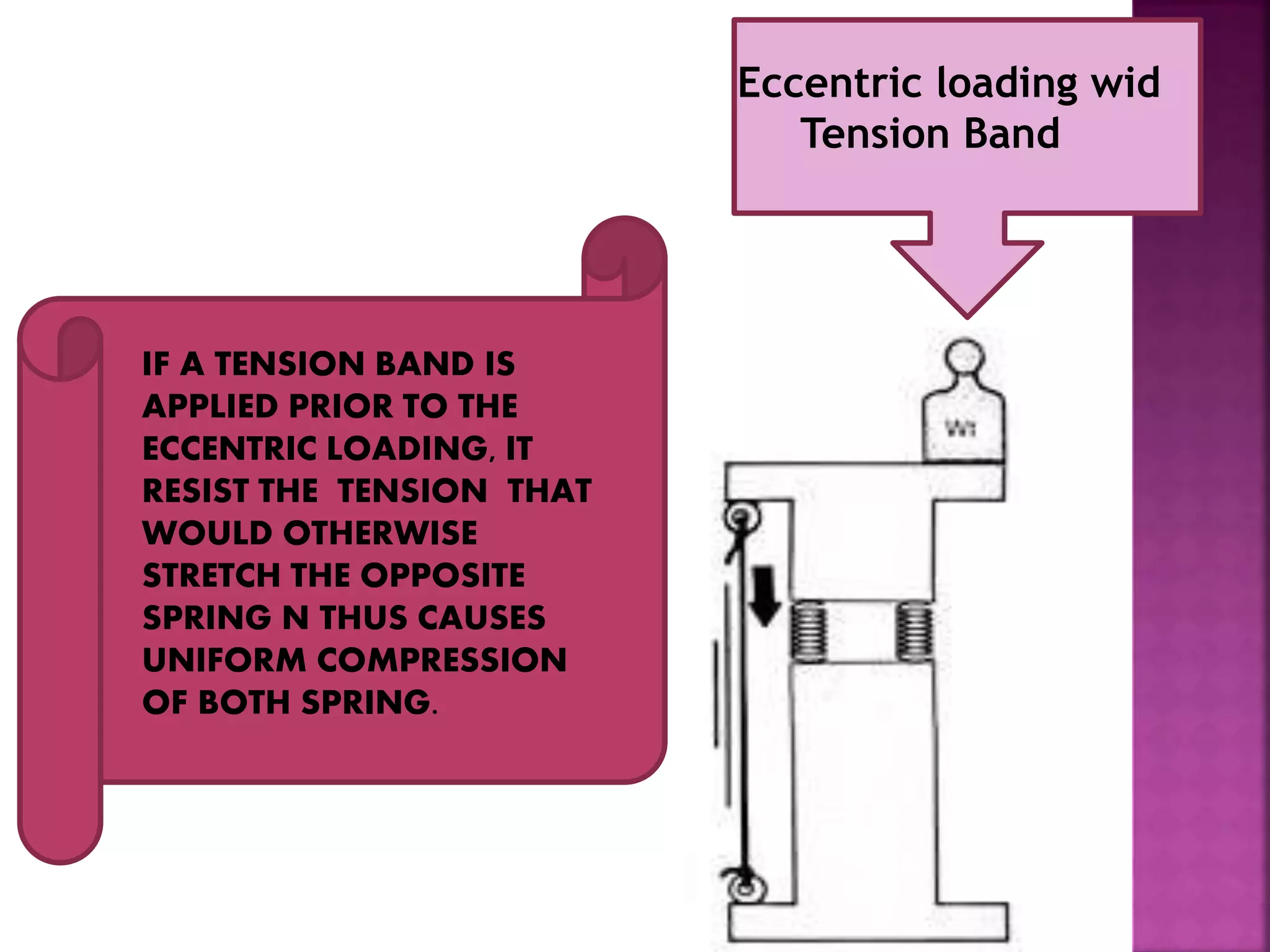
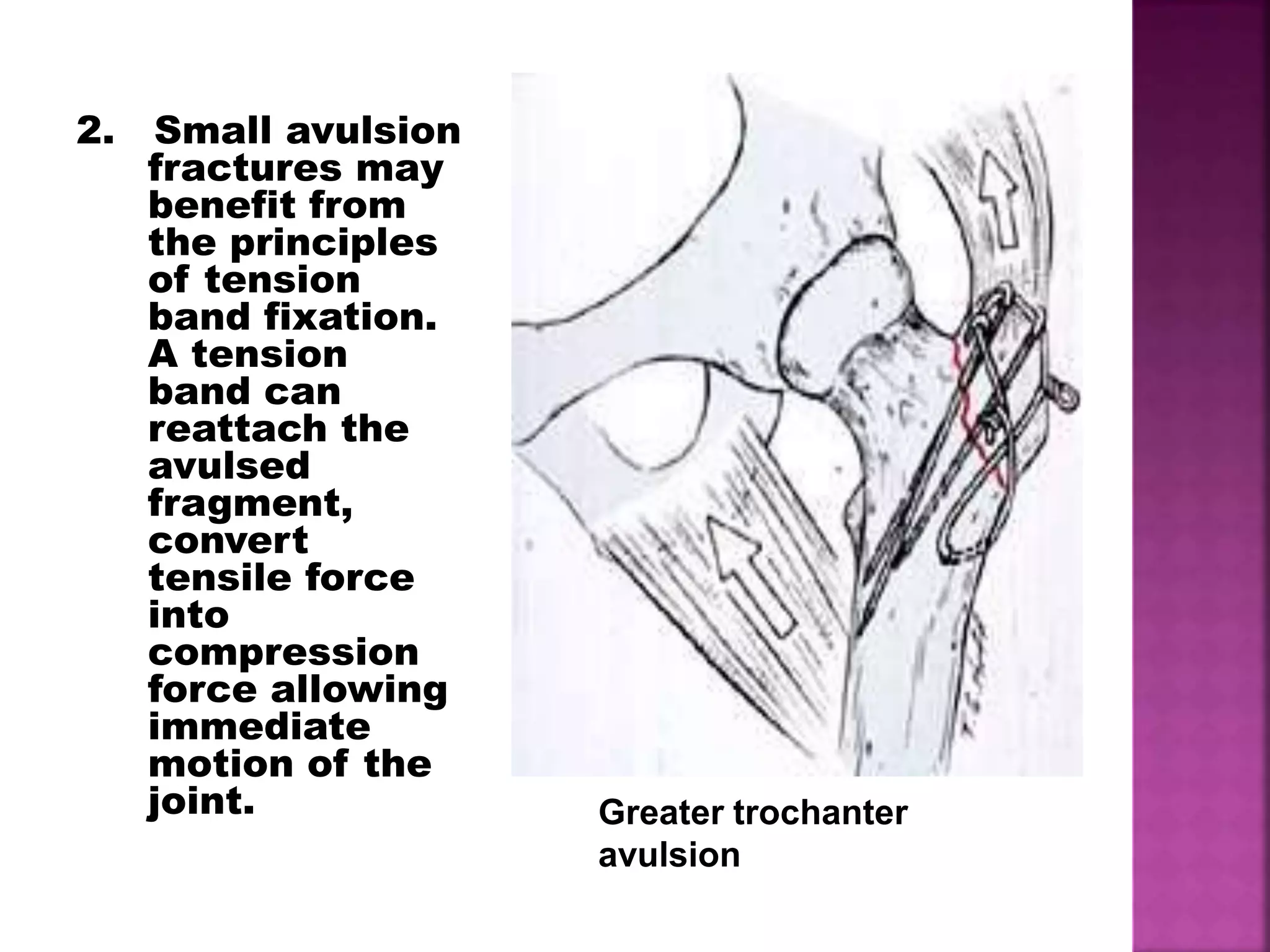
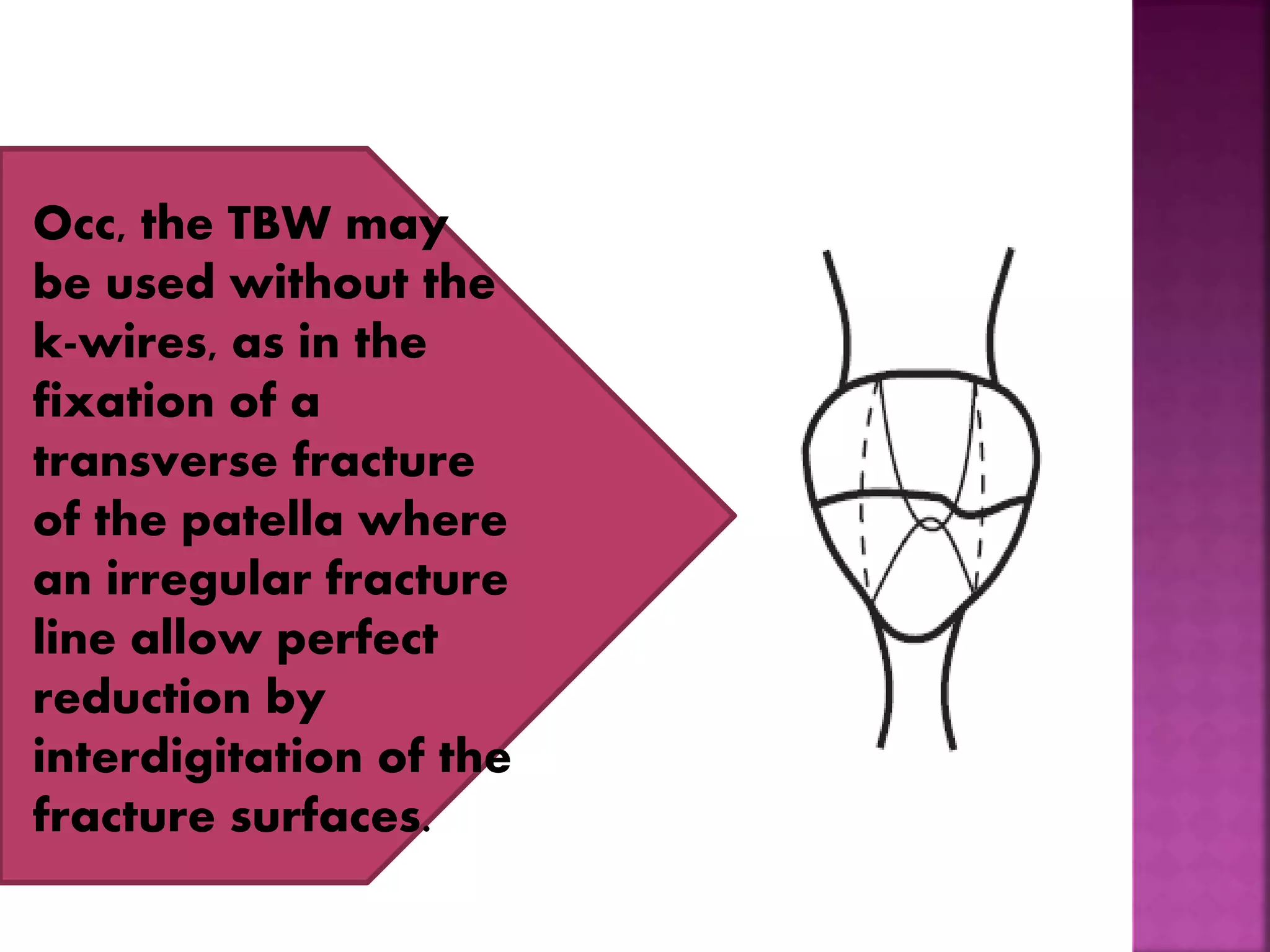
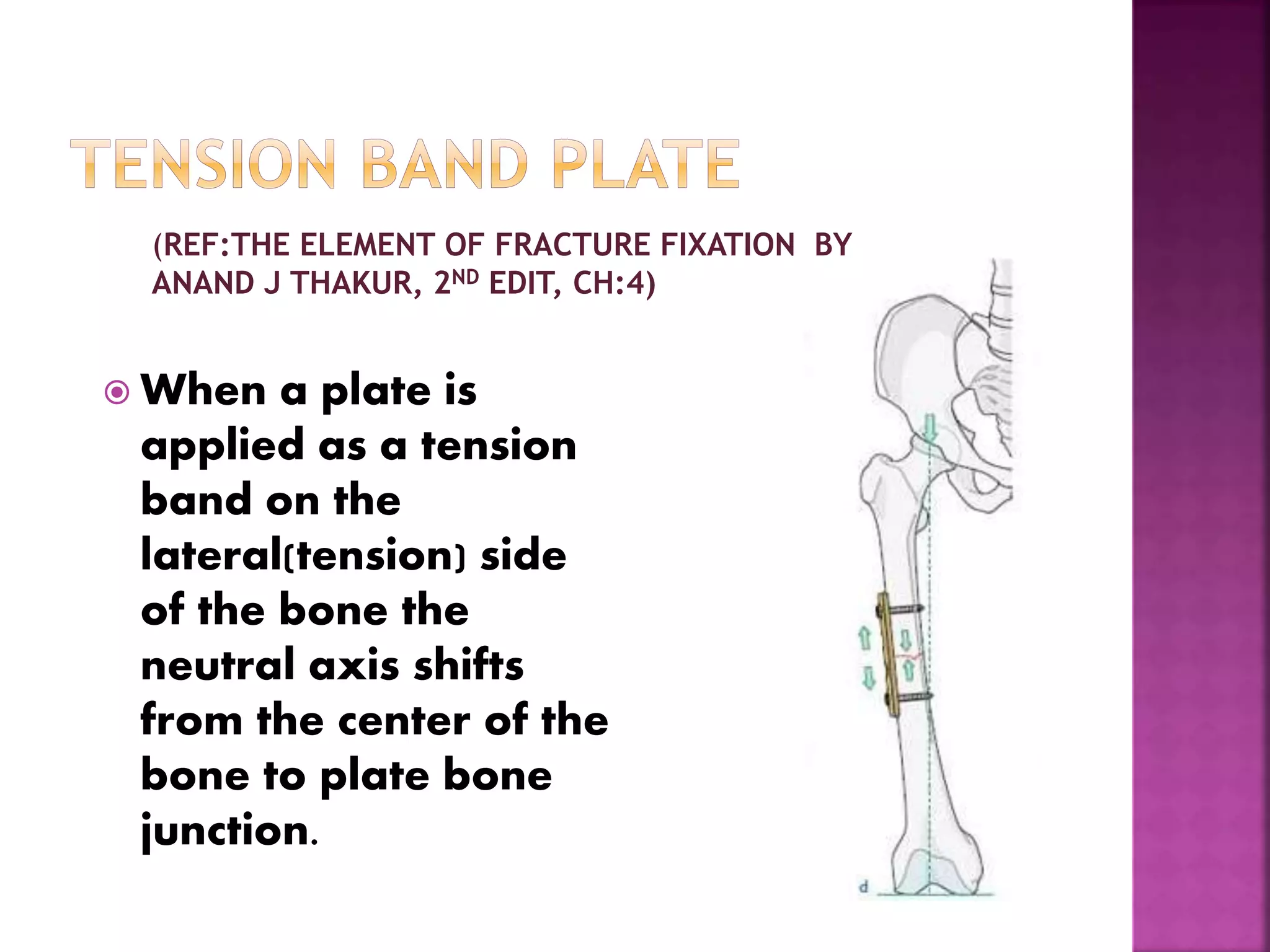
1. The tension band technique converts tensile forces into compressive forces through the application of a tension band on the tension side of a bone.
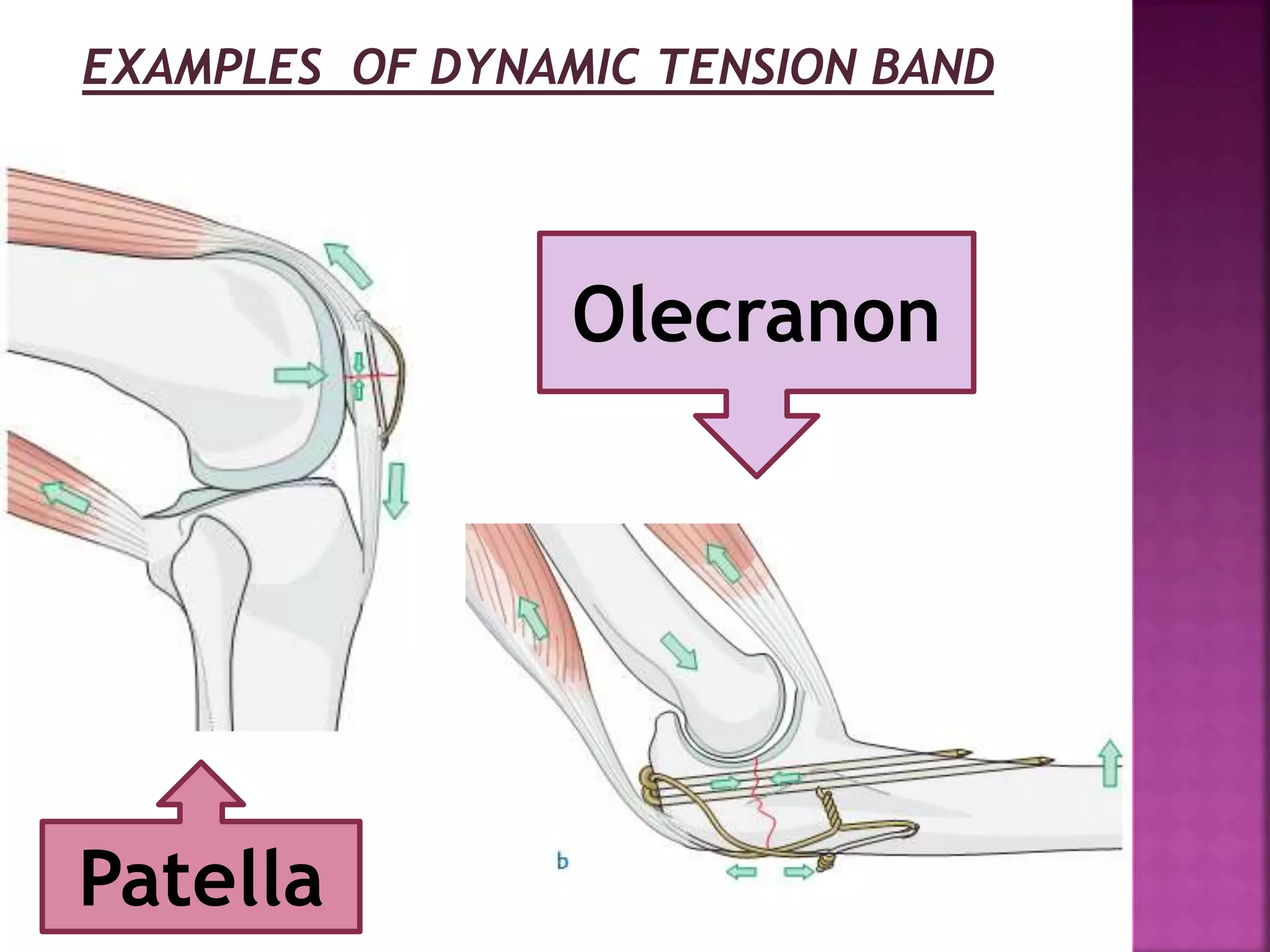
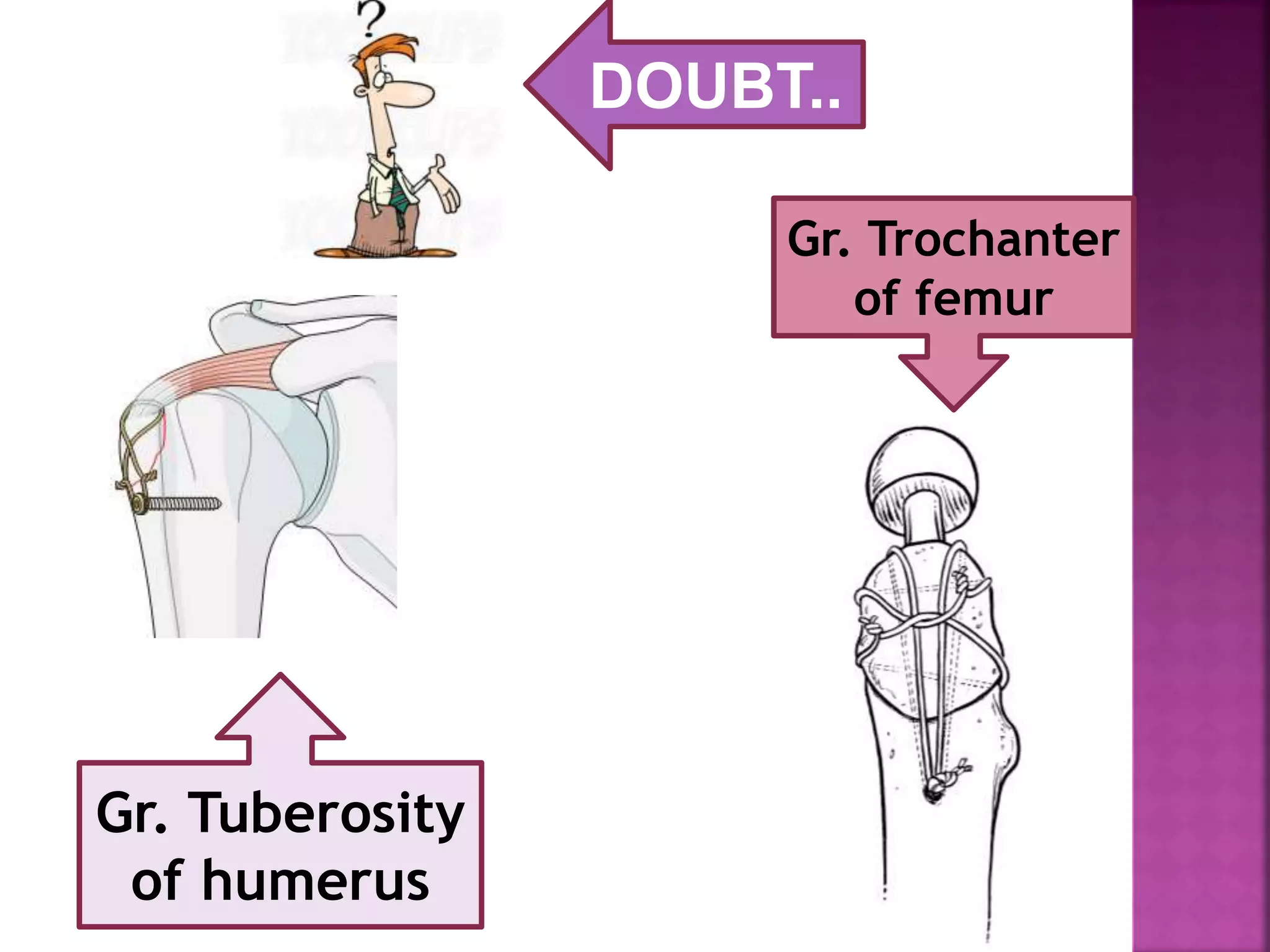
2. Examples of where tension band fixation is commonly used include patella and olecranon fractures, as well as fractures of the greater tuberosity and greater trochanter.
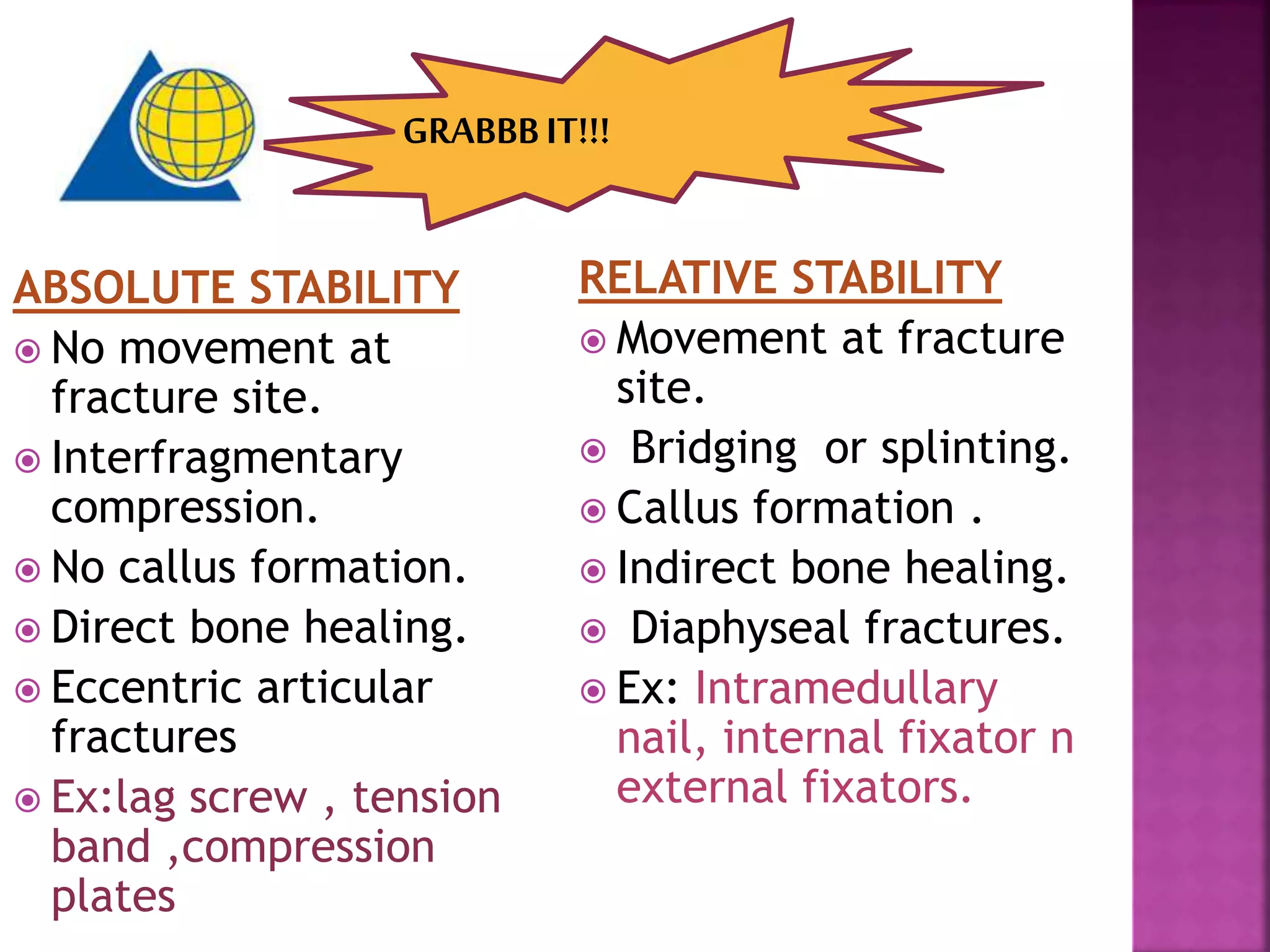
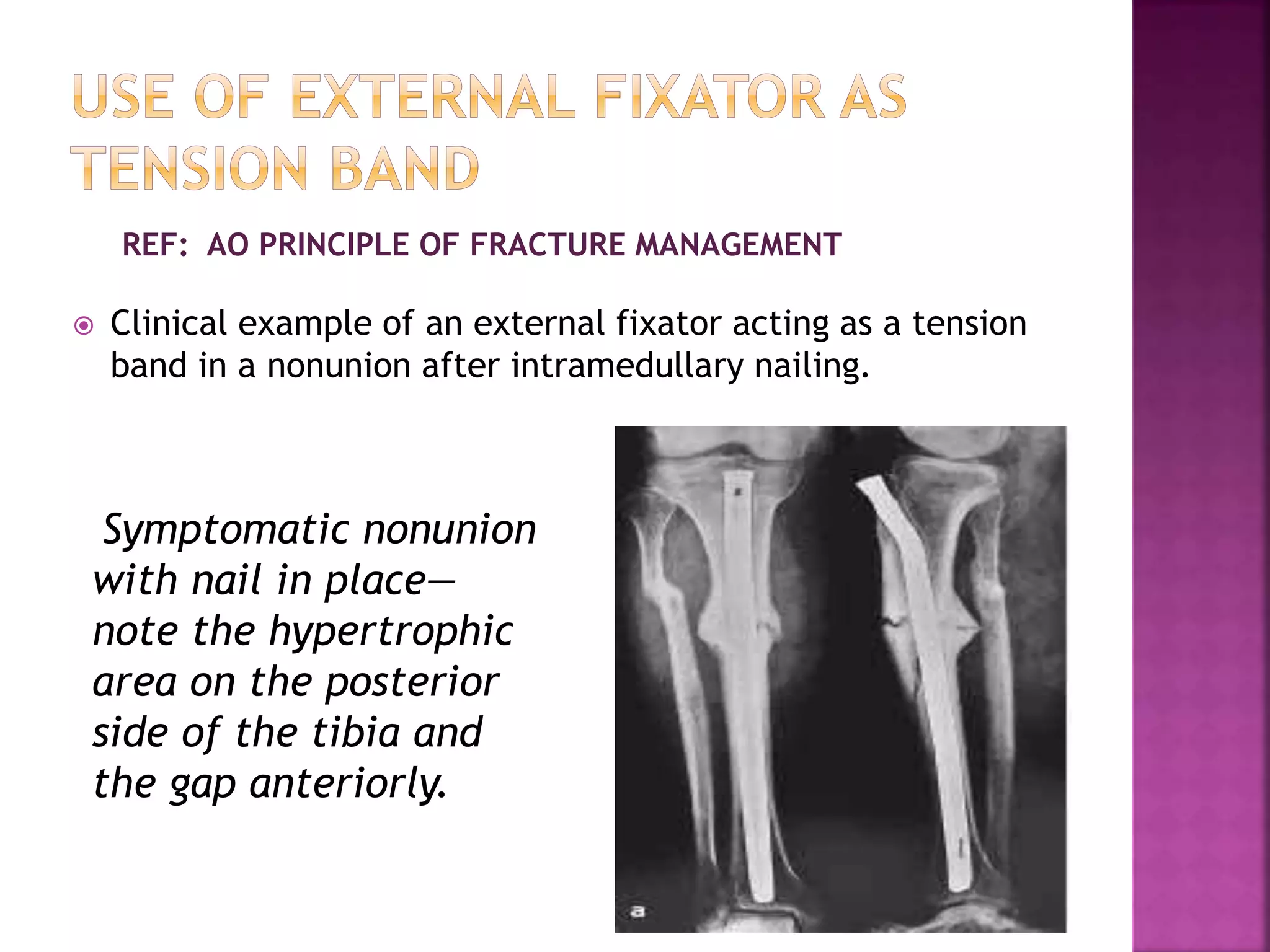
3. Tension band wiring, plating, and external fixation can all function as tension bands by applying a compressive force across a fracture to promote healing.